[ad_1]
WHAT IS ALREADY KNOWN ON THIS TOPIC
-
To effectively tackle the issue of health workers’ (HWs) migration from low/middle-income countries (LMICs) and improve health systems, robust data, especially related to the drivers of migration or non-migration, are needed.
-
Although LMICs are most impacted, to date, no systematic review has exclusively studied these groups of countries to understand the key drivers of emigration, migration intention or non-migration.
WHAT THIS STUDY ADDS
-
We report, to our knowledge, the first systematic review that rigorously assessed the drivers of migration/intention to migrate across all human resources for health cadres from LMICs covering the last five decades.
-
We analysed the changing trends and factors influencing HWs’ migration from LMICs over time, and examined the reasons for non-migration among those who remain in their source countries.
-
We used two policy-relevant conceptual frameworks to synthesise and categorise the drivers of HWs’ migration from LMICs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Introduction
Human resources for health (HRH) play a crucial role in the functioning of health systems and have been demonstrated to impact population-level health outcomes.1–3 A 2022 Global Burden of Disease Study estimated that a minimum of 20.7 physicians, 70.6 nurses and midwives, 8.2 dental personnel and 9.4 pharmaceutical personnel per 10 000 population would be required globally to achieve universal health coverage.4 Regarding absolute numbers, the minimum thresholds fell short by 6.4 million physicians, 30.6 million nurses, 3.3 million dental personnel and 2.9 million pharmaceutical personnel.4 Furthermore, to achieve the health-related sustainable development goals (SDGs), the WHO recommended a health workforce density of 4.45 per 1000 population.5 Nevertheless, a growing concern is that by 2030, a shortage of 18 million HRH will occur, primarily in low/middle-income countries (LMICs) of Southeast Asia and sub-Saharan Africa.6 Recognising such shortfalls, SDG 3c aims to significantly boost health financing and enhance the training, recruitment, development and retention of HRH in LMICs.7 However, the emigration of HRH exacerbates the existing workforce shortages in their home countries, leading to reduced access to healthcare, increased healthcare costs and adverse health outcomes for the population.8 9
The migration of HRH from LMICs is a pressing global health issue with significant implications for both sending and receiving countries.10 It is influenced by a complex interplay of push and pull factors at the individual and systemic levels.11–13 At the individual level, factors such as better job opportunities, improved working conditions, higher salaries and better career prospects can act as drivers for migration.14 15 At the systemic level, weak health systems, limited professional development opportunities, political instability and poor governance can push HRH to seek employment elsewhere.11 12 14 Additionally, the global distribution of health workers is influenced by macro-level factors such as economic globalisation and international trade agreements,16 17 which can exacerbate workforce migration from LMICs. A comprehensive understanding of these drivers is essential for developing effective policies to retain health workers in their home countries.
To effectively tackle the issue of HRH migration from LMICs and improve health systems, robust data, especially related to the drivers of migration or non-migration, are needed to inform measures taken by governments and organisations such as the WHO. Unfortunately, systematic review data on the drivers of HRH migration are sparse, with the existing reviews having a limited scope related to LMIC settings.18–21 Previous systematic reviews on the drivers of HRH migration have only examined specific categories of HRH,18 21 such as nurses or physicians, or have restricted their studies to a particular country, especially the UK.18 19 21 Although LMICs are most impacted, to date, no systematic review has exclusively studied these groups of countries to understand the key drivers of emigration, migration intention or non-migration. Furthermore, previous systematic reviews have not analysed the changing trends and factors influencing HRH migration from LMICs over time, nor have they explored the reasons for non-migration among those HRH who remain in their source countries.
This systematic review, therefore, aims to determine the drivers of health workers’ out-migration, intention to migrate and non-migration from LMICs. The specific objectives are: to document publication trends and identify the cadres of health workers studied, their source and destination countries, and to categorise drivers of HRH out-migration, migration intention and non-migration from LMICs using a relevant policy-oriented framework. This review will also determine if there have been changes in the drivers of HRH out-migration or intention to migrate from LMICs over the past decades and compare drivers between HRH with migration intention and those who have already migrated, between cadre and between geographical regions within LMICs.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.22 The review protocol was registered with PROSPERO (CRD42022334283) and published a priori in a peer-reviewed journal.23 The review process did not deviate from the previously published protocol. However, we updated the original protocol to include studies that modelled drivers of HRH migration as they were found to be a rich source of macro-level drivers of migration.
Information sources and search strategy
We systematically searched five electronic databases: Ovid MEDLINE, EMBASE, CINAHL, Global Health and Web of Science. We also examined the reference list of retrieved items to identify additional articles further. The search strategy was developed based on several variants of the key concepts from the study aim: health workers, low-and middle-income countries and migration. The search strategy was developed, refined and implemented using a three-stage approach. In the first stage, a preliminary search was conducted in the MEDLINE database using key concepts, and the search terms were refined based on the titles and indexing terms of the retrieved items. The refined search strategy was adapted and applied to all the databases in the second stage. In the final stage, the reference list of included full-text papers was searched for additional articles not found in the database search. During the search, we truncated text words and applied wildcards to enable the retrieval of relevant articles that used different spellings for the same word. In addition, we combined text words and Medical Subject Headings terms using Boolean operators. All databases were searched in August 2022. The complete search strategy employed across all five databases is available in online supplemental table 1.
Eligibility criteria
Primary studies, including those with quantitative, qualitative or mixed-methods, and studies based on secondary data with the following specific characteristics were included in the review: (a) focused on any category of HRH from any LMIC (ie, low-income, lower middle-income and upper middle-income economies) based on the 2020 World Bank classification24; (b) assessed HRH migration or intention to migrate; (c) reported any determinant of HRH migration; and (d) published in English or French language. We did not apply any date restriction for the included studies. We excluded systematic or scoping reviews, journal correspondence or commentary on HRH migration or intention to migrate. Also, studies reporting data from HRH from LMICs who trained and have only worked in high-income countries were excluded because we considered that their experience might not reflect those of their colleagues who trained or have worked in LMICs.
Study selection
We exported all the retrieved titles into the EndNote V.20 (Clarivate Philadelphia, Pennsylvania, USA) reference management software to remove duplicates. After deduplication in EndNote, the records were transferred to Rayyan (a web-based application for screening articles of systematic review)25 for blinded screening of the title and abstract by three independent reviewers. Any study that did not meet the prespecified eligibility criteria was excluded, and the reasons were documented. All disagreements regarding the inclusion of studies were resolved by a consensus after discussion by the three independent reviewers. Whenever the three initial reviewers failed to reach a consensus, a fourth research team member acted as an arbiter. Following the title and abstract screening, full-text articles were retrieved, and when not found, we explored options such as interlibrary loans. However, we did not contact the authors to request access.
Data extraction
Data extraction was conducted using a standardised data extraction form developed to reflect the sequence of variables required from the included studies. Three authors independently pilot-tested the data extraction form using 20 randomly selected full-text articles, and the form was subsequently refined based on feedback from the pilot testing process. The articles were divided among three teams, with three reviewers in each team. Two reviewers extracted each article, which the third reviewer verified to confirm the accuracy of the extracted variables. The extracted variables are listed in online supplemental table 2, and the merging decisions for conceptually similar variables.
Risk of bias in individual studies
Two reviewers independently evaluated the methodological quality of the included primary studies. The mixed-methods appraisal tool (MMAT) was used for the evaluation as it is a single tool that can handle different study designs, including quantitative, qualitative and mixed-methods studies.26 The MMAT was chosen because it addresses the difficulties of using multiple appraisal tools for different study designs in a single review. It is well validated and focuses on five core criteria that are relevant to each study design, rated on a scale of ‘yes’, ‘no’ or ‘can’t tell’ to provide consistent appraisals. To summarise the overall quality of the included studies (online supplemental figure 1A,B), we used the descriptors ‘low’, ‘medium’ and ‘high’. A study was classified as ‘high quality’ if all five criteria were rated as ‘yes’. Studies that met three to four criteria were considered ‘medium quality’, while those that met one or two criteria were deemed ‘low quality’. Any disagreements during the appraisal process were resolved through consultation with a third team member. No studies were excluded based on methodological quality to ensure a comprehensive data representation from as many countries as possible.
Synthesis of results
Given the heterogeneity of the included studies regarding their study design, population and outcome of interest, we did not conduct a meta-analysis. Instead, a narrative synthesis was used to summarise the results. Based on two frameworks, we synthesised the drivers of HRH migration or intention to migrate. The first framework is the migration theory of push and pull factors, which refers to factors that drive people to leave their home country (push) and factors that attract them to a foreign country (pull).27 The second is Young’s framework which categorised these push and pull factors into three levels: macro-level (global and national factors), meso-level (professional factors) and micro-level (personal factors).28
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
The initial search produced 27 542 publications, of which 21 593 were unique after deduplication. After reviewing the titles and abstracts, 21 373 articles were removed. The full texts of the remaining 220 articles were obtained, but 12 were inaccessible and 114 were not eligible for inclusion. An additional 25 articles were found in the reference list; however, only 13 were eligible for inclusion. In the end, 107 articles11 29–134 were eligible for the final analysis, as shown in the PRISMA flow chart in figure 1. Out of the included articles, 82 were single-country studies that focused on 26 countries. The remaining 25 articles were based on data collected from multiple LMICs. Table 1 shows the summary of key article characteristics, while the assessment of the methodological quality of the articles is included as online supplemental figure 1A,B.
Characteristics of the 107 included studies in the systematic review on health workers’ migration or intention to migrate from low/middle-income countries
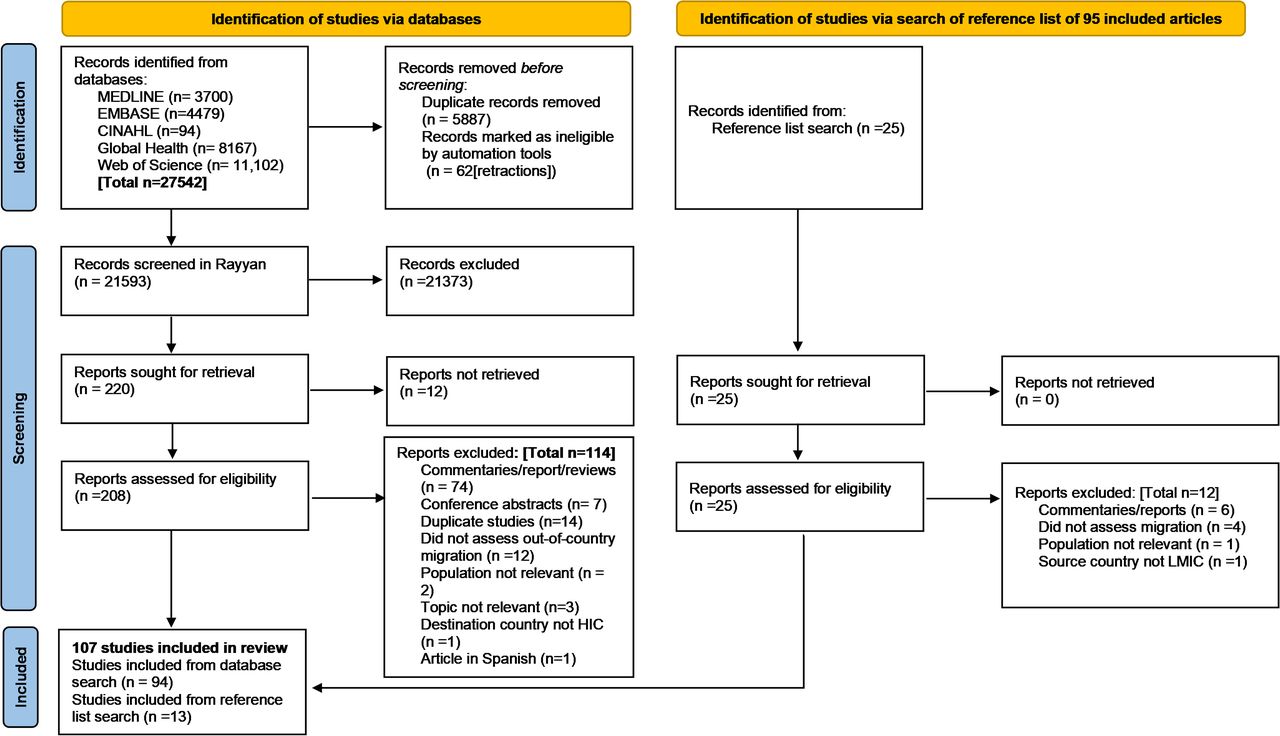
Flow chart showing identification, screening and selection process of included studies. HIC, high-income country; LMIC, low/middle-income country.
Publication trend, the cadres of HRH studied, the source and the destination countries
Few studies on HRH migration were published before 2004 (figure 2A). However, the publication of articles on the topic gained momentum in 2004, peaking in 2014 with 13 articles37 56 60 86 106–111 123 129 134 published that year. Most articles focused on doctors and nurses, representing 64.5% and 54.2% of the included articles, respectively (figure 2B). The source countries of HRH migration are shown in figure 2C, with 18.7% (20 of 107) of the articles covering data from multiple countries. The top source countries, as determined by studies with single-country data, are South Africa (15.9% (17 of 107) of articles), India (12.1% (13 of 107)) and the Philippines (6.5% (7 of 107)). The WHO African Region had the highest number of source studies from single-source countries (27.1% (29 of 107)) compared with other LMIC regions.34 36 41 42 52 57 59 60 62 64 66 69 75–77 82 85 88 92 95 97–99 122 124 129 130 133 The UK is the leading destination country, with 44.9% (48 of 107) of the articles studied, followed closely by the USA at 42% (45 of 107) (figure 2D). Australia and Canada both had 32.7% representation in the articles. Other destination countries include the United Arab Emirates with 11.2% representation, New Zealand with 9.3% and Saudi Arabia with 8.4% representation in the articles.
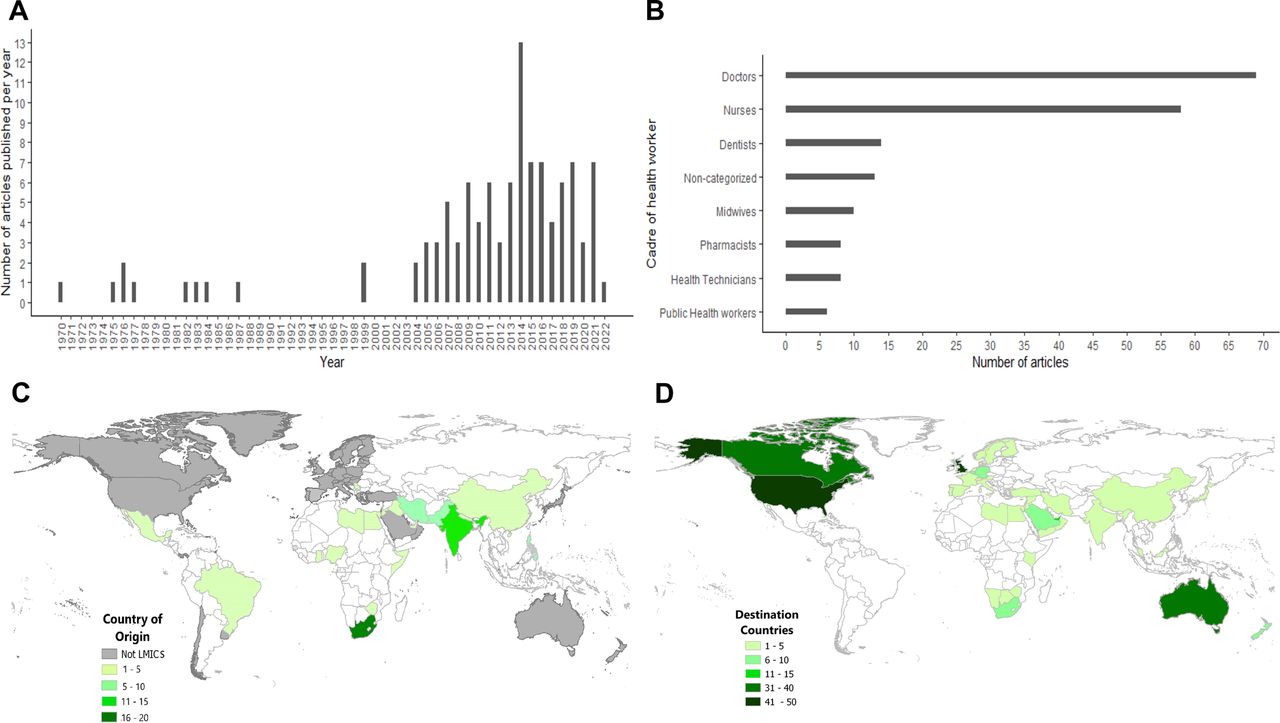
(A) Publication trends on HRH migration; (B) the cadre of the health workforce studies; (C) the source country and (D) destination countries HRH emigrated to or intend to migrate to, 1970–2022. Non-categorised represents studies where the cadre of HRH was not explicitly stated. Source countries shown on the map are from studies focusing on a single country rather than multiple LMICs. HRH, human resources for health; LMICs, low/middle-income countries.
Drivers of out-migration, intention to migrate and non-migration
Overall, the most common drivers were the macro-level (global and national) and meso-level (professional) factors. Remuneration and security were the most common macro-level factors driving HRH migration from LMICs, with 83.2% and 58.9% of studies, respectively, identifying these factors (figure 3A). The main drivers at the meso-level were career prospects (81.3%), a good working environment (63.6%) and job satisfaction (57.9%). The most cited micro-level factors (ie, personal factors) were family ties (61.6%) and improved quality of life (69.7%).

The local push factors were the most reported and mirrored the foreign pull factors. Poor pay, work environment, career development, infrastructure and job satisfaction were the most listed local push factors. In contrast, financial incentives, a good work environment and career development were the topmost foreign pull factors (figure 3B). The most common local pull factors (ie, drivers of non-migration) were family ties, job satisfaction and advancing age. In contrast, the most common foreign push factors were sociocultural barriers and the cost of migration.
The trends in the drivers of migration and non-migration of HRH from LMICs
Between 1970 and 2022, financial incentives (pay-related drivers) and career advancement (ie, opportunities or lack thereof) have consistently been reported as drivers of HRH migration in included articles. These two drivers were evident as foreign pull and local push factors, as depicted in figure 4. However, from around the early 2000s until 2022, other drivers such as a better quality of life, working conditions (good or poor), insecurity/security and unfavourable sociopolitical situations became more frequently cited as reasons for HRH to leave their source countries or be attracted to the destination countries.

Trends in the drivers of health workforce migration in low/middle-income countries, 1970–2022. Per cent (%) of articles represents the proportion of articles each year that reported a particular driver.
Evaluating drivers of migration by migration status and geographical regions
Overall, the key factors driving migration were similar for HRH who have already migrated and those who plan to migrate (figure 5A). For example, local push factors such as poor sociopolitical situations, poor pay and lack of job satisfaction were reported by a similar number of articles in both categories of HRH. Similarly, foreign pull factors such as having a family member abroad, good career opportunities, financial incentives and security were also equally reported in both groups (figure 5A). In addition, the key drivers were consistent across geographical regions, as the same drivers were consistently reported in articles from different regions, particularly in Africa, the Eastern Mediterranean and Southeast Asia (figure 5B).

Comparison of drivers of migration by (A) migration status and (B) geographical regions across low/middle-income countries, 1970–2022. Geographical regions are based on the WHO geographical regions. AFRO, African Region; AMRO, Region of the Americas; EMRO, Eastern Mediterranean Region; EURO, European Region; SEAR, South East Asian Region; WPR, Western Pacific Region.
Discussion
HRH migration from LMICs is a significant challenge to achieving SDG 3, as adequate health workforce-to-patient ratios are essential for promoting well-being for all ages.5 The already deficient HRH in most LMICs is associated with poor health outcomes, and continuous emigration/intention to migrate further exacerbates this problem. We report, to our knowledge, the first systematic review that rigorously assessed the drivers of migration/intention to migrate across all HRH cadres from LMICs covering the last five decades. Publications on HRH migration/intention to migrate gained momentum in the early 2000s, the majority focusing on doctors and nurses, with the UK and USA as the top destination countries. The major drivers of this phenomenon were macro-level (national) and meso-level (professional) factors and have remained relatively unchanged over the last five decades. The top macro-level and meso-level drivers include remuneration, security (or lack thereof), career prospects, job satisfaction and working environment-related factors. These drivers do not appear to differ among HRH who have migrated and those with intention to migrate or across geographical regions in LMICs.
The primary research into HRH migration was sporadic between the 1970s and the late 1990s. Most of the studies in the era sought to capture the experiences of doctors or nurses in their destination countries, including culture shocks, acceptance and adaptations in the workplace, and migration drivers.41 45 59 61 78 79 120 122 127 128 131 However, in the early 2000s, we found a surge in research on HRH migration that peaked in 2014 and covered a wider range of healthcare workers, including those who had already migrated and those planning to do so. This shift coincided with the growing global concern about the adverse effects of a chronic global shortage of well-trained HRH, which was most acutely felt in the countries that need them most. In 2006, the WHO World Health Report was dedicated to HRH—launching a Decade of Human Resources for Health.135 In 2010, another global call to action was made during the WHO World Health Assembly when the Code of Practice on the international recruitment of health personnel was adopted.136 These events may have contributed to the increased publications that sought to understand the drivers of HRH migration and intention to migrate.
We found that the LMICs with the highest number of studies were South Africa, India and the Philippines. These countries are situated in regions persistently dealing with conflicts and social inequality.137 138 Furthermore, some of these countries also struggle with other issues such as corruption, unemployment, rising xenophobia attacks, and murder targeting migrants and minority groups.139 140 Sadly, as the health workforce may not be immune from these dangers, they often leave these countries entirely for their safety. Thus, it is unsurprising that security and poor working environment were key drivers of migration/intention to migrate reported among HRH from these countries. We found that the prospect of a safer environment, opportunities for career advancement and conducive immigration policies with a promise of improved quality of life motivated HRH to leave their home countries. The UK, USA, Canada and Australia were the most preferred destination countries. National health scheme implementation, ageing populations and a shortage of trained HRH in these countries may have created a demand for foreign-trained HRH to fill gaps in the local workforce.135 While the WHO advocates controlled migration of HRH with a minimal negative impact on source countries’ health systems,136 progress also depends on how top destination countries implement such guidelines.19 This review shows that most of the included studies focused on doctors and nurses, which is unsurprising since these cadres are the largest and disproportionately represented in the health workforce of many countries globally.5 6 This is especially true in LMICs, where healthcare roles are less diverse than in wealthier nations. Since doctors and nurses are responsible for diagnosing, treating and caring for patients, their scarcity can have detrimental effects on health outcomes.
This review identified remuneration-related issues and future career prospects as critical drivers of HRH emigration or intention to migrate, operating at macro-level and meso-level, respectively. At the micro-level, family ties in the destination country and the quest for improved quality of life were the major drivers of migration. Our findings are consistent with prior research demonstrating that financial safety needs, opportunities for professional development through training and research, and the desire for improved quality of life for HRH and their families are critical drivers of HRH emigration.19 141–143 These findings highlight the complex, multilayered, inter-related factors that may influence HRH emigration or intention to migrate. The implications of these findings are far-reaching and underscore the need for increased investment in LMIC health systems from state and non-state actors to support the welfare and career aspirations of the health workforce. By improving their welfare, access to training and opportunities for professional growth, LMICs can build a more stable and sustainable health workforce that meets their populations’ needs. In addition, policies that improve the overall quality of life in LMICs would have a positive spillover effect in reducing the migration of HRH.144 We also found that the key drivers of non-migration (ie, local pull factors) of health professionals from LMICs were personal (micro-level) factors such as advancing age and family ties, similar to previous research.20 It is likely that the relative stability of family structures, the communal nature of societies in many LMIC contexts and the relative lack of additional benefit to older persons who migrate partly explain this finding. Nevertheless, personal issues of advancing age and family ties are not affected by policies aimed at halting HRH emigration from LMICs.
Overall, the key drivers of HRH emigration/intention to migrate have remained relatively unchanged over the last five decades and are similar among HRH with intention to migrate and those who already migrated and across geographical regions. This finding highlights the need for countries and development partners to rethink the past and ongoing approaches implemented to address the drivers of HRH emigration from LMICs. Despite the worrying nature of the issue, there is a unique opportunity for countries to collaborate and create a co-learning space to develop more robust strategies to retain HRH, as their similarity across regions suggests that effective strategies implemented in one LMIC may be applicable to others.
This review is subject to some limitations. First, some source countries such as South Africa, India and the Philippines were disproportionately represented, accounting for over one-third (34.5%) of all the included studies, thus, may have skewed our findings. However, the fact that we included a large number (107) of studies, most of which were of medium quality, means that our findings may largely be representative. Second, the majority of included studies (64.5%) focused solely on doctors, and an additional 54.2% focused on nurses, with limited focus on other essential cadres of HRH. Moreover, many of these studies did not differentiate the drivers of HRH emigration between the different cadres. Consequently, we could not examine whether the drivers differed across cadres as we initially proposed in the study protocol. Third, the included studies were mainly cross-sectional, thus, did not examine the changing trend of a particular cohort of HRH over time. Trends in a single cohort may be more insightful and relevant to decision-making and policy formulation. Future research should consider following a specific cohort to investigate whether the drivers of emigration, intention to migrate and non-migration change over time. Such studies should aim to include LMICs that were either under-represented or not represented in this review to provide a more balanced representation, as the drivers may have differed significantly. Additionally, studies should be designed to compare the drivers of migration and non-migration between different health workforce categories.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge Dr Ekhosuehi T Agho for his contribution to the development of the protocol for this systematic review.
[ad_2]
Source link