Tips for Buying the Best Kitchen Plastic Products for your Home
Would you like to store your food in a reasonable manner? In the event that you do, you don’t have to stress over its capacity since you have kitchen plastic family things on your side.
While purchasing kitchen plastic storage boxes for your home, here are a few hints to consider to pick the best ones:
Quality and Security: Search for kitchen plastic storage boxes that are produced using top notch materials and fulfill wellbeing guidelines. Check for names demonstrating that the items are sans bpa and food-grade. This guarantees that they are alright for putting away and taking care of food.
Toughness: Decide on kitchen plastic items that are solid and dependable. Search for items produced using strong materials that can endure everyday use, dishwashing, and temperature varieties without breaking or distorting.
Usefulness: Think about the planned utilization of the plastic items and pick ones that satisfy your particular requirements. For instance, in the event that you really want food capacity compartments, search for ones with secure covers and impermeable seals. Assuming you really want utensils, consider ones that have ergonomic handles for agreeable use.
Simple Upkeep: Select kitchen plastic items that are not difficult to clean and keep up with. Search for items that are dishwasher-protected or simple to hand wash. Keep away from items that have convoluted or difficult to-arrive at regions that can trap food buildup or become hard to clean.
Heat Obstruction: Assuming you intend to involve plastic storage boxes for microwave or broiler purposes, guarantee that they are microwave-safe and can endure high temperatures. Search for items with clear guidelines demonstrating their intensity obstruction abilities.
Size and Limit: Consider the size and limit of the plastic items in view of your stockpiling needs or how much food you normally handle. Pick food capacity compartments in various sizes to oblige different piece sizes or extras.
Right now where the costs of any things are contacting the sky; everyone is searching for a reasonable and effective answer for their consistently to day issue. The cash you make is certainly going to assist you with getting the food yet this cash will likewise assist you with putting away your food or increment their life expectancy and that is just conceivable assuming you contribute it on the right things.
Having plastic storage boxes in your kitchen would assist you with putting away your food. In any case, this is the one method for using plastic items in your family. In the event that you don’t have the foggiest idea how to get it and from where to get it, you don’t need to stressed over it since you have us on your side.
We supplies plastic storage boxes that are tough, reasonable and are liberated from synthetics. In this blog, we will uncover numerous things in regards to family kitchen plastic things. So remain with us till the finish to be aware of it.
Kinds of kitchen plastic storage boxes
Prior to purchasing any item you should have a legitimate information about it. The plastic storage boxes utilized in our kitchens are not made of just a single sort of plastics. Every item has various plastics utilized in them. There are numerous items produced using various plastics that are being utilized in the kitchen so we should uncover the items made up from these plastics.
Cutting board: This plastic made item is a high priority thing in your kitchen. Prior to setting up any feast, we start with this item. This item is exceptionally reasonable and contains non-slip surfaces. This item is made up from polypropylene.
Garbage cans: This plastic garbage cans is made up from Polycarbonate (PC) and is additionally among one of the most amazing plastic item. It’s absolutely lightweight and sturdy.
Food Capacity Compartments: There are numerous plastic stockpiling boxes in Pakistan that is chiefly made to store the extra food; you can likewise name it food capacity holders. These are light in weight and Take less space.
Kitchen baskets: This item is additionally produced using different plastics like high-thickness polyethylene (HDPE) and polypropylene (PP).
Blending bowls: This plastic food compartment is produced using Polycarbonate (PC) and Melamine. This item is mostly used to blend any dry items in your kitchen.
What are Different Types of Liability Accounts
Basically every business manages liabilities, or things that it owes or has acquired. The comprehensive definition of liabilities states that liabilities are likely future sacrifices of economic benefits resulting from a company’s current obligations to transfer assets or provide services to other companies in the future as a result of previous transactions or events. However, referring to liabilities as debt is a much more intuitive description. In order to acquire resources and fund operations, businesses frequently seek funding from third parties. The lender might hold the option to either seize the acquiring business’ resources or make the borrower offer them to reimburse any remaining obligation.
To represent the creditor’s claim to the borrower’s capital in the event that debts are not paid, liability accounts are recorded on the right side of the borrower company’s balance sheet. Through the transfer of economic benefits in the form of money, goods, or services, these debts are paid off over time. The aat level 2 course accounting equation requires that the total amount of liabilities equal the total amount of assets and equity.
Resources = Liabilities + Value
Normal Sorts of Liabilities
There are two primary sorts of liabilities, current and non-current. A current liability is the first type, and it is expected to be paid off within one year or the operating cycle, whichever comes first. As a result, they are more commonly referred to as short-term liabilities. a non-current liability, on the other hand, has a longer duration. The borrower has over a year to pay off their debt. These debts are also referred to as long-term or fixed liabilities. The various kinds of liability accounts that fall under these two categories are outlined below.
Current Liabilities
Overdraft occurs when a company borrows money from a bank by overdrawing its account, taking out more money than the account is worth, and then paying back the difference to the bank. There is interest on the credit, and there is regularly a charge for each overdraft.
When a company purchases goods or inputs on an account and must repay them, this is called accounts payable.
Taxes Payable – for the purpose of collecting sales taxes and deductions for employees;
Any wages that the business owes to its employees but has not yet paid;
Gathered Costs – when a business or association represents costs that it will pay off at future dates;
Customer prepayments are money paid by customers in exchange for services or products from the company;
Current Portion of Long-Term Debt: a portion of debt with an overall maturity of more than a year; Interest Payable: any interest on loans that has been accrued but has not been paid as of the date on the balance sheet. portion is due within a year.
Deferred or unearned revenue is when a business sells goods or services to a customer who pays for them but never receives them. Those products and services are still owed to the customer.
A fixed-liability mortgage is a loan used to buy new property or expand an existing one;
Loans for automobiles and equipment typically involve significant upfront costs that must be paid back over time;
Notes Payable are the company’s equity or debt securities;
Deferred Tax Liabilities arise when an accounting period’s income differs from the taxable amount reported on the return;
Annuity Commitments – cash that must be represented to make future benefits installments;
Other Long-Term Debt: borrowings that have to be paid back in full in more than a year.
Contingent liability
A contingent liability is a third, less common type of liability in addition to the ones mentioned above. These debts are contingent on upcoming outcomes, or contingencies. If both of the following conditions are satisfied, a contingent liability can be established:
Although their name suggests something negative, liabilities are actually important aspects of enterprise management. The outcome is likely. The cost can be reasonably estimated. They are vital to arranging fruitful tasks and making esteem.
For instance, organizations regularly acquire cash to subsidize activities, pay for huge developments, and smooth out exchanges with different organizations. When these debts are not managed well, they become a problem, which can lead to financial decline, problems with solvency, and, in the worst cases, bankruptcy. To keep away from these issues, entrepreneurs ought to get comfortable with the sorts of liabilities and how they are assessed during the bookkeeping cycle.
Top benefits of a steel and glass Conservatory
The production of steel and glass has improved over time, laying the groundwork for the development of winter garden designs into increasingly fascinating and modern structures. The greenhouse architecture of the nineteenth and twentieth centuries was characterized from an aesthetic standpoint by a vast repertoire of shapes and decorations, influenced by the neoclassical, neo-gothic, and Moorish styles, thanks to new and increasingly particular metal bearing structures.
We quickly developed winter garden Timber windows birmingham conservatories as a result of the success of greenhouses, the desire to enjoy them throughout the year, and the pleasure of interacting with the lush green world. These structures consequently wound up turning into a fundamental part or an expansion of the house.
As a matter of fact, it was exactly the chance of having the option to partake in the outside space in spite of horrible weather patterns influencing the interest of the first class of the time.
These days, studios aren’t made exclusively in steel and glass yet additionally in different materials like wood and aluminum. However, the strengths of the metal winter gardens have already been highlighted: solidity, fire resistance, and the columns and structures’ overall lightness.
As a matter of fact, steel has numerous characteristics that meet the prerequisites of the development of a colder time of year garden. There is no question about the predominance of centers in steel and glass contrasted with different materials.
Why? Read on.
The advantages of steel conservatories
A winter garden’s metal structure provides stability and strength. Before receiving a specific powder-coating preparation treatment to prevent corrosion and for a long-lasting effect, each of the steel components goes through a complicated and elaborate cutting, welding, and assembly process.
However, what are the benefits of constructing conservatories out of steel?
Steel winter gardens are well-liked for their durability, as was mentioned at the beginning of the article. In point of fact, steel is a sturdy yet simple metal to work with, making it an excellent choice for the construction of conservatories, where strength and robustness are crucial.
For instance, a conservatory made of steel and glass would be ideal for housing a large living room with a dining room next to it because it would be able to provide the structural support that is required for spaces this size.
Conservatories made of steel are more durable and resistant
Metal is able to withstand the elements despite being exposed to weathering. Problems with maintenance and repair are few and far between with metal frame constructions because they are so strong and long-lasting.
Setting up a construction requires the readiness of the establishment and significantly longer establishments times than the get together of an iron and glass structure. It is sufficient to install metal plinths as a base for the construction of a steel conservatory without constructing a foundation, leaving the ground unaltered, if the dimensions permit it. Additionally, the bolt-fixed structure can be assembled and disassembled for repositioning elsewhere.
Because steel is a malleable material, winter gardens made of it can be folded and shaped in a variety of ways. Conservatories can be designed in any style and perfectly match any structure, regardless of its design or architecture, thanks to these features.
Top 10 Steps To Achieve Stunning Results With Fluid Audio Mastering
There’s a world of possibilities waiting for you in fluid audio mastering. Mastering is crucial for giving your tracks that final polish, ensuring they not only sound great but also compete on a professional level. In this guide, you’ll discover the top 10 steps you can take to enhance your mastering workflow and achieve stunning results that elevate your music. By following these steps, you’ll ensure your projects sound polished and impactful, ultimately captivating your audience and making your music shine.
Quality Source Material
For stunning audio mastering results, it is crucial to start with quality source material. This foundational step ensures that all subsequent processing and enhancements are built upon a solid base, ultimately leading to a polished final product that stands out in any listening environment.
Use High-Resolution Audio
Quality source material necessitates the use of high-resolution audio. By opting for formats like WAV or FLAC with higher bit depths and sample rates, you allow your audio tracks to retain a richer level of detail, which is vital during the mastering process.
Select the Best Takes
Source material is only as strong as its individual components, making the selection of the best takes critical in achieving exceptional results. Choosing the right performances not only enhances the overall quality of your audio but also contributes to a more cohesive and professional-sounding final mix. Ensure that you thoroughly review and compare each take, focusing on elements like emotion, timing, and technical proficiency before finalizing your selections. This attention to detail will pay off when it comes time for mastering, as your chosen takes will reflect the highest standard possible.
Takes that stand out should resonate with clarity and emotion, freeing you from the pitfalls of weak performances that could diminish your final output. Engaging in a careful selection process will maximize the potential of your audio. Keep in mind, one exceptional take can elevate your project significantly, while a mediocre performance can overshadow your hard work in the mixing phase. So take the time needed to ensure that only your best takes make the final cut.
Proper Mix Balance
If you want to achieve stunning results with fluid audio mastering, focusing on achieving a proper mix balance is important. A well-balanced mix allows each element of your track to shine, maintaining clarity and dynamic range. Without this balance, even the most meticulous mastering process may fall flat, leading to a less impactful final product.
Level Adjustments Matter
Some key level adjustments can dramatically improve your mix. By carefully adjusting the volume levels of individual tracks, you create a cohesive sound where each element is heard distinctly, preventing one section from overpowering another. This attention to level is crucial for achieving a professional sound.
Frequency Distribution Crucial
Proper frequency distribution ensures that your mix doesn’t become muddy and that it translates well across various playback systems. Any imbalances in frequency can lead to a significant loss of clarity and energy in your track. By addressing these distributions, you allow your mix to breathe and shine with vitality. You’ll want to pay close attention to avoid frequency clashes—overlapping frequencies from multiple instruments can create a chaotic sound that can be particularly dangerous. Aim for a distinct presence in low, mid, and high ranges to achieve a dynamic mix that positively enhances your track’s overall impact.
Use Reference Tracks
Even the most skilled mastering engineers benefit from using reference tracks. They serve as a benchmark for your mixes, allowing you to identify areas for improvement and ensure your sound matches professional quality. This practice can significantly enhance the overall impact and clarity of your audio, making it imperative for achieving stunning results in fluid audio mastering.
Compare with Professional Mixes
You’ll want to compare your tracks with professional mixes that resonate with your desired sound. This process can pinpoint specific areas where your mix may be lacking. Below is a table detailing the elements to focus on when comparing:
| EQ Balance | Assess how frequencies are distributed and adjust accordingly. |
| Dynamic Range | Examine the loudness and softness throughout the track. |
| Spatial Imaging | Evaluate how elements are placed in the stereo field. |
| tonal richness | Pay attention to warmth and body in your mix. |
Identify Tonal Balance
Identify the tonal balance of your mix by analyzing how the low, mid, and high frequencies interact. Understanding this balance is crucial in achieving a mix that sounds full and well-rounded while avoiding muddiness or harshness.
It is imperative to have a clear tonal balance in your mix. Use your reference tracks to identify if certain frequencies are overpowering others. When using a reference track, ensure that your lows are defined but not boomy, your mids are clear, and the highs are smooth without any unwanted sibilance. This balance will provide a professional polish to your track and make it more enjoyable for the listener. Regularly revisiting and adjusting these aspects can lead to a more cohesive and compelling final product.
Consistent Monitoring Environment
Unlike many other aspects of audio mastering, achieving stunning results heavily relies on a consistent monitoring environment. Your monitors will dictate how you perceive and, ultimately, how you adjust your mix. When creating or mastering music, having a stable listening environment is paramount to avoid distortion, misunderstanding of frequency balance, or confusing sound dimensions.
Room Acoustics Optimized
One of the first steps to optimizing your monitoring environment is to ensure that your room acoustics are well-treated. This involves addressing issues such as flutter echoes and standing waves to create a flatter frequency response. Proper acoustic panels, bass traps, and diffusion techniques can significantly improve your listening conditions.
Reliable Speakers and Headphones
If you want to achieve audiophile standards in your mastering process, it’s crucial that you invest in reliable speakers and headphones. The quality of audio gear will directly influence how accurately you can interpret what you’re working on.
Monitoring with high-quality gear ensures that your sound translates well across different playback systems. Your speakers should offer flat frequency response, allowing you to hear every detail without exaggerated highs or lows. Meanwhile, a solid pair of headphones can help you isolate elements in your mix. Always calibrate and familiarize yourself with your equipment; this way, you’ll avoid the danger of misjudging frequencies that could lead to devastating errors in your final output.
Employ Dynamic Range
Once again, mastering the dynamic range of your audio tracks is crucial for achieving a professional sound. The dynamic range refers to the difference between the quietest and loudest parts of your audio. When you skillfully employ dynamic range, you make your music more engaging and impactful. Do not forget, it’s not just about loudness; it’s about creating a sound that resonates.
Maintain Volume Control
Now, ensuring you maintain optimal volume control throughout your mix can make a substantial difference in your final product. By carefully balancing levels, you create a coherent sound that draws listeners in without overwhelming them. This careful management helps retain the expressive qualities of your music.
Avoid Excessive Compression
Dynamic range can be significantly impacted by how you choose to use compression in your mastering process. Excessive compression can cause your tracks to lose their natural dynamics, resulting in a flat and lifeless sound. Instead, aim to apply compression judiciously to enhance clarity and punch, while still allowing room for the music to breathe.
Any overuse of compression can lead to detrimental outcomes such as reduced depth and emotional impact in your audio. When you over-compress, you risk squashing the life out of your sound, rendering it monotonous and exhausting for the listener. Maintain a balance: ensure that your peaks are controlled but always leave space for those quieter moments that can add texture and richness to your track. Do not forget, a well-mastered audio track should feel alive, with dynamics that invite the listener in.
Frequency Analysis Tools
After you have prepared your audio for mastering, employing frequency analysis tools can elevate your results significantly. These tools help you visualize and understand the frequency content of your track, guiding you to make informed decisions while mastering your audio.
Visualize the Spectrum
To truly appreciate the complexities of your mix, utilizing a spectrum analyzer allows you to see the frequency distribution of your audio. This visual representation can help you pinpoint areas of resonance or imbalance, ensuring that your final master has a balanced and polished sound.
Identify Problematic Frequencies
The second crucial step is to identify any problematic frequencies that may cause issues in your mix. Problematic frequencies can lead to muddiness, harshness, or an overall lack of clarity, which can be detrimental to the quality of your final product.
This process involves using your frequency analysis tools to closely examine the spectrum for peaks and dips. Peaks can indicate frequencies that are overly present, making the mix sound cluttered, while dips might show areas where your track lacks fullness. By addressing these issues—such as by applying EQ adjustments—you can enhance your mix’s clarity and coherence, ultimately leading to a more professional and polished audio master.
Utilize EQ Effectively
Despite the complexity that can arise in the mixing process, utilizing EQ effectively is paramount for achieving stunning audio results. Proper application of EQ can enhance clarity, reduce muddiness, and create a well-defined sound that stands out in any genre.
Enhance Clarity and Separation
Separation is crucial in mixing; it allows each element of your track to be heard distinctly. By utilizing EQ to carve out frequencies for different instruments, you can enhance clarity and ensure that every component occupies its own sonic space. This technique creates a more balanced mix where elements like vocals, guitars, and drums shine without overpowering one another.
Reduce Muddiness or Harshness
Effectively reducing muddiness or harshness in your mix can transform an otherwise cluttered sound into a polished masterpiece. This involves identifying troublesome frequencies and utilizing your EQ to selectively cut or attenuate them. Aim to bring out the warmth of your bass elements while ensuring your high frequencies are crisp yet not abrasive.
Clarity in your track is achieved by recognizing and addressing problematic frequency zones. Investigate the lower mid-range, usually between 200-500 Hz, where muddiness often lies. A gentle cut in this area can greatly enhance the overall definition of your mix. Conversely, focus on the 2-4 kHz range if you find your mix sounding too harsh. By precisely sculpting your EQ, you’ll not only create balance but also breathe new life into your tracks.
Apply Limiting Judiciously
Many audio enthusiasts strive for a polished and professional sound, making it important to use limiting carefully. Limiting can help you achieve a loud master without sacrificing quality, but overusing it can lead to a lifeless mix. Ensuring that you apply limiting judiciously will make a significant difference in the overall quality of your track.
Control Peaks Smartly
To effectively control the peaks of your audio, utilize a transparent limiter that allows you to tame excessive transients without compromising the signal’s integrity. Keep an eye on the gain reduction meter to ensure you’re not squashing your mix too much, as this could lead to unwanted artifacts and distortion.
Preserve Overall Dynamics
Overall, maintaining the dynamic range of your audio is vital for retaining its emotional impact. When applying limiting, aim to highlight the musicality of your track while avoiding a flat or compressed sound. This ensures that your music retains its expressiveness and dynamics, which are crucial for engaging your listeners.
A good balance is key; dynamic range is what keeps your listeners engaged and allows the music to breathe. By using limiting to control peaks without over-compressing, you can maintain the natural ebb and flow of your audio. This approach not only enhances the listening experience but also preserves the essence of your artistry, providing a more rewarding journey for your audience.
Final Listening Checks
All your hard work culminates in the final listening checks, where you can ensure everything is in perfect order before release. This stage is critical for catching any overlooked details that could impact the listening experience.
Test on Multiple Systems
On conducting tests across different playback systems, including headphones, studio monitors, and consumer speakers, you can accurately gauge how your mastered audio translates in various environments. This step is vital to ensure your work sounds great, whether in a professional studio or on average home equipment.
Gather Feedback from Peers
Feedback from trusted peers can provide you with fresh perspectives and constructive criticism. Consider sharing your master with fellow musicians, producers, or sound engineers to gain insights into aspects that might need refining. Their experience can help highlight critical issues you might have missed, ensuring your final product is as polished as possible.
Peers can offer valuable input as they may notice subtle nuances in your audio that you have become desensitized to over time. Their feedback can include aspects like tonal balance, dynamic range, and overall coherence. It’s crucial to be open to their insights and ready to implement any necessary changes. Engaging in this collaborative process can ultimately elevate your work and lead to greater listener satisfaction.
Summing up
Considering all points, by following the top 10 steps to achieve stunning results with fluid audio mastering, you can elevate your music to professional standards. Implementing best practices such as establishing a clear reference, using quality monitors, and paying attention to your project’s dynamics will enhance your overall sound. Do not forget, mastering is an art that requires both technical skills and creative intuition, so don’t hesitate to experiment while keeping your goals in mind. Your dedication to these steps will undoubtedly lead to impressive results and a polished final product.
Missing in action: a scoping review of gender as the overlooked component in decolonial discourses
[ad_1]
WHAT IS ALREADY KNOWN ON THIS TOPIC
WHAT THIS STUDY ADDS
-
Colonisation was both racialised and gendered, resulting in what many have referred to as a sexual and racial hierarchy through which power is distributed. The gendered nature of colonisation is insufficiently acknowledged and addressed in the decolonising global health literature, leading decolonial initiatives and reforms to overlook and leave unchecked the perpetuation of racialised notions of gender, a crucial element of coloniality which continues to cause power asymmetries.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
-
An awareness of where and how gender appears in the decolonising global health literature with regard to research, practice and policy should encourage global health colleagues to be more intentional and inclusive in their work; failure to counter and confront the multiheaded beast of coloniality in its totality will otherwise allow gender-based inequities to flourish when reform efforts remain inadequate.
Introduction: exploring the gendered dimensions of colonialism and coloniality
Colonisation marked the advent of global capitalism, transporting structures of domination and subjugation across borders and oceans under the guise of ideological righteousness. To enable the large-scale exploitation of peoples and extraction of resources, a sexual and racial hierarchy was imposed by colonial forces to create and perpetuate significant power asymmetries, dehumanise large swathes of the world’s population and reduce them to (re)productive labour in service of empires.1 2 As Allotey and Reidpath state in correspondence with Abimbola and Pai, ‘Decolonisation is fundamentally about redressing inequity and power imbalance. It cannot be achieved without also addressing gender inequity, racism, and other forms of structural violence’.3 4 However, as calls to decolonise global health continue to gain momentum, we note with concern the sidelining of gender in discourses within this space and the closing window of opportunity to embed intersectionality and allyship within the decolonising global health movement.
For this study, the working operationalisation of ‘gender’ goes beyond the binary, recognising both the full spectrum of gender identities and the structural manifestations of gender as a construct that operates at individual, institutional and systemic levels, resulting in inequities. While scholarship on decolonising global health does not entirely overlook the presence of patriarchal privilege,5 the connection between gender inequities in health and the colonial construction of gender is often left either unsaid or uninterrogated. This presents a significant and ongoing impediment to the advancement of gender equality and health equity as part of the 2030 Agenda for Sustainable Development, as neither goal can be achieved so long as coloniality and the resultant power asymmetries that drive gender inequalities and health inequities remain unaddressed.
Lugones1 2 6 outlines a ‘coloniality of gender’ which positions gender as a colonial construct introduced as part of broader efforts to categorise and control colonised peoples. Crucially, she points out that ‘[c]olonialism did not impose precolonial, European gender arrangements on the colonised’1; rather, a new system that took into account both gender and race was created, one which privileged European men for both their gender and race, European women for their race, colonised men for their gender and colonised women for neither. Put simply, Lugones tells us that as a direct consequence of colonisation, new gender hierarchies, differentials and relations were forced on colonised societies, where they then intersected with constructions of race to produce power dynamics and inequities that remain alive and well today.1
Lugones’ work expands on Quijano and Ennis’7 coloniality framework and the larger body of literature on decoloniality, which states ‘that even with un-colonialism, coloniality remains’8 and operates through three intersecting sites: power, being and knowledge. Quijano further conceptualised four processes through which coloniality exerts its power: ‘control of the economy, control of authority, control of gender and sexuality, and control of knowledge and subjectivity’.9 However, the control of gender and sexuality is frequently overlooked in analyses grounded in the three sites of coloniality, including those by Quijano.
If coloniality is understood as an invisible power structure that sustains colonial relations of exploitation and domination long after the end of physical colonisation, decolonial analysis and action must include and confront the gendered dimension of coloniality and its ongoing impacts on health. Not doing so risks failing to address the root causes of gender-based inequalities across the global health ecosystem and facilitating the perpetuation and manifestation of racialised notions of gender, from the domination of global health leadership by white men from high-income countries10 11 to disparities in healthcare provision between Aboriginal women and their non-Aboriginal or male counterparts.12 Whether one chooses decoloniality, feminism or a broader lens of equity as their entry point to assessments of power inequities in global health, it is crucial to develop an understanding of how local notions of gender and the resultant power dynamics and differentials, whether inherited from or shaped by colonialism, interact with other factors such as race, class and ability to affect implementation, access and uptake.
Previous works in the space of gender and health have identified coloniality in conjunction with racism and sexism as ‘interconnected structures of power’.13 Building on the work of Lugones and other decolonial feminist scholars,14 15 we argue that racism and sexism are not only interconnected with coloniality and each other but are, in fact, different manifestations of the same root problem: a fundamental imbalance of power achieved by and perpetuated through the creation of hierarchies. We call not for gender to be ‘added’ to decolonial analysis and action but for it to be recognised as a core component of the colonial project which must be addressed in all decolonial attempts and initiatives which seek to challenge power inequities in all their manifestations. As a starting point, we offer this scoping review locating where and how interrogations of gendered power inequities are taking place in the decolonising global health literature.
Methods: a scoping review in search of gender within the decolonising literature
To better understand where, why and how (in/frequently) gender appears in decolonising discourses, we undertook a scoping review of the decolonising global health literature. A literature search of the Scopus and PubMed online databases was conducted to identify peer-reviewed papers with the search terms “(decoloni* or de-coloni*) OR (neocolonial or neo-colonial) AND ‘global health’” in their title, abstract or keywords published by December 2022. The search was restricted to papers in English as this is the working language of both reviewers. Unfortunately, the restriction of the search to English excluded discussions that are known to be occurring in French, Spanish, Portuguese, German, Chinese and others.16 Other exclusion criteria included the following: not focused on global health, not focused on colonialism, no full text available and not a peer-reviewed article. To ensure a thorough review of the relevant literature, no start date exclusion criterion was applied; however, the cut-off date for new papers was the end of December 2022 to facilitate analysis. No registered review protocol is available.
Search results were uploaded into the Covidence review platform and deduplicated; at this stage, papers were not yet excluded based on interaction with gender. The initial filtration based on the review of the title and abstract was conducted by a single reviewer (ELMR). We defined global health as ‘an area of study, research and practice that places a priority on improving health and achieving equity in health for all people worldwide’.17 18 Papers that met the inclusion criteria explicitly discussed colonialism, the need for decolonisation or decoloniality and/or neocoloniality with respect to global health. In total, 167 papers progressed to the data charting stage, with the following information extracted:
-
Bibliographic: Title, journal, publication year, article type, authorship (first, last and middle) and authorship affiliation with low-income and middle-income countries or former colonies.
-
Content: Main theme(s), definition of (de)colonisation/coloniality, articulation of problem, articulation of solution, mention of specific colonised populations, intersection with gender and details of gender discussion (if applicable).
Full-text review and extraction were completed by ELMR and TN-A, with each paper in the database independently reviewed by both, followed by inductive thematic coding of the subset of papers that had any mention of gender, gendered population groups, gendered participation or gender of researcher(s). The initial coding round was conducted separately, with the coding frame further refined following discussions between ELMR and TN-A. The coding process allowed for a single paper to contain multiple themes. A second round of coding using the refined frame was undertaken by ELMR and TN-A to further categorise papers into two sub-subsets: those that included gender but did not interrogate its intersection with coloniality and those that did.
Results: where and how does gender appear in the decolonising global health literature?
Of the total 167 papers in our review (see figure 1), 53 (32%) engaged with gender; engagement with gender includes the use of the word ‘gender’ and its derivatives, mention of any gender identities or discussion of themes and topics related to gender, gender dynamics, gender norms and gender inequalities. A summary of the topics discussed by these 53 papers follows (see online supplemental file 1 for the complete dataset).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of the literature search.
Papers that discussed (de)coloniality and engaged with gender covered a range of global health issues, from specific topic areas to broader concerns about governance and knowledge. Six papers focused on sexual and reproductive health and rights19–24 with a further two papers specifically on maternal health,25 26 while five papers focused on mental health,27–31 three papers discussed health in humanitarian settings,30 32 33 two papers focused on planetary health34 35 and one paper focused on non-communicable diseases.36 Five papers had a focus on pandemics, ranging from prevention37 to transmission38 to response,39–41 and one highlighted the challenges surrounding the production and distribution of vaccines.42 Nine papers had a service delivery focus which analysed the impact of (de)coloniality on service provision21 25 39 43 44 and service providers,23 36 45 46 while seven analysed community engagement in research methods40 44 47–50 and programme design.38 Seven papers concentrated on Indigenous health, of which four studied the health of Indigenous peoples39 40 43 46 and three discussed Indigenous conceptions of health.34 37 49
The impact of persistent coloniality in global health research has been a notable feature of the broader decolonising global health discourse. Of the 53 papers that discussed (de)coloniality and gender, 18 articles focused on global health research encompassing research partnerships,51–54 underlying epistemologies45 55 56 and methodological approaches,32 33 40 47 50 through to publication.57 Some of these papers were focused at the level of the individual,58 while others addressed structural and systemic factors driving inequity.59–62 Nine papers reviewed and/or called for changes to global health63 and medical education27 28 61 64 and curricula65–67 and reflected how current educational approaches ‘hold back health equity’.68
Finally, six papers discussed changes to the broader global health architecture, exploring who holds power60 69 70 and who can dictate agendas,20 39 51 while two focused specifically on changing the approach to global health policy.59 71
For the purposes of this review, we were interested in papers that explicitly engaged with the intersection of gender and coloniality. Of the 53 papers that engaged with gender, just under half (49%, n=26) met this criterion, in contrast to 27 (51%) papers that simply mentioned gender, either referring to gender inequalities or discussing gender in the study design (see table 1).
The final set of 53 papers reviewed, categorised by nature of engagement with gender
Below, we present an analysis of the 26 papers that examined the intersection of gender and coloniality.
Discussion: what does the literature tell us about the gendered dimensions of decolonising global health?
Through our analysis of the 26 papers that presented a clear link between gender and coloniality, four key themes were identified. The first two themes address the coloniality of being and knowledge; in other words, how colonial constructs continue to shape the ways in which we assign value to ourselves and each other as human beings, as well as the hierarchy by which we evaluate and assign legitimacy to different epistemologies and ways of knowing. The latter two themes discuss the implementation impacts of coloniality on health policies and programmes and explore the value of applying a decolonial gender lens in such analyses to inform action for change.
Intersecting colonial constructs of race and gender continue to drive contemporary inequities
Colonialism oversaw the institution of a racialised and gendered colonial hierarchy which “supposed the innate superiority of Christian European white males over every ‘other’ group”;20 37 56 60 68 eleven papers19 20 26 29 34 35 37 39 56 60 68 in our analysis discussed the ramifications of this hierarchisation of society based on the assumed value of individuals. Within this hierarchy, colonised subjects were framed as ‘less than fully rational, closer to nature and thus less than fully human’56 with gender overlayed. The native male body was viewed as an uncontrollable vessel of sexual urges in need of subjugation and control,19 while the native female body was a casualty of the ‘redemptive sacrifice’ required to bring about civilisation and thus reduced to a site of (re)productive labour.34
Through and due to this enactment of a racialised and gendered hierarchy, ‘a series of codes, norms, typographies and ideas concerning sexuality’20 rooted in Eurocentric ideals were introduced and continue to drive gender inequities in health even today. Some papers explored the pathologisation of gender identities and sexual orientations that sit outside of what Lugones describes as the ‘modern/colonial gender system’, driven by a ‘colonial, Eurocentered capitalist construction’ of gender and characterised by ‘biological dimorphism (and) the patriarchal and heterosexual organisation of relations’.1 Others examined the ways in which academia and medical science have replaced European religion as the primary arbiters of these ‘norms’ which designate colonised subjects and their descendants as ‘lesser’ gendered beings of colour. For example, Sastry and Dutta share how in Bangladesh, the dehumanising trope of ‘the uncontrollable sexual urges of the native male body’ was perpetuated by (and to some extent, informed and drove) programmes advocating for male sterilisation funded by the U.S. President’s Emergency Plan for AIDS Relief.19 This coloniality of (gendered) being alienates individuals, silences identities and replaces worldviews in a destructive and harmful process that continues today.68
Gendered notions of expertise and evidence perpetuate colonial conceptions of knowledge
Coloniality is an inherently destructive endeavour, predicated on the eradication and replacement of one or many things with a hegemonic ‘default’. Eight papers21 35 36 45 48 55 60 69 discussed how coloniality put into place a hierarchy of knowledge and its gendered dimensions and impacts. This hierarchy of knowledge is a clear extension of the racialised and gendered hierarchy which governed colonial and colonised societies, with white men identified as ‘the only legitimate purveyors’60 of knowledge, a knowledge that is derived from Eurocentric epistemology. This imposition of ‘the coloniser’s model of the world’69 as the default has left in its wake a trail of ‘silenced subaltern voices’,45 including colonised women and LGBTQIA communities who are often relegated to being ‘objects’ of science rather than experts and practitioners55 and ‘systematically denied platforms’6 for ‘knowledge production and idea generation’.48
While the arbiters of knowledge remain largely unchanged from colonial times, with a majority of global health journals not only headquartered in the North but also managed by editors based in the North,72 they continue to wield this power not only through the violent and visible destruction of epistemologies but through domination over knowledge production, dissemination and validation. Within global health, the continued existence of this hierarchy has significant consequences in research, policy and practice as it reinforces the hegemony of Eurocentric ways of knowing, gatekeeps priority-setting power and silences voices deemed to be inferior in decision-making fora.21 45 55 Even for those seeking to interrogate and challenge gendered inequalities in health, Somerville and Munguambe caution that there is an ever-present risk of falling ‘into the same problematic space of taking as starting point conceptualisations of gender that are born of a theoretical tradition that is firmly Western’, which runs counter to contemporary understandings of gender as a colonial construct and risks creating perceptions of gender equality as a ‘neocolonial imposition’.36
Coloniality drives gendered impacts of health programmes and policies
The Eurocentric worldview which determines, among other things, prevailing paradigms in how the bodies of ‘others’ are viewed, has impacted the way that global health has been, is and might be implemented. 10 papers19 21–23 26 36 44 59 64 71 in our study explored these facets in more detail, illustrating how ‘ethnic stereotypes and gendered racial ideas’ affect programme design, targeted populations and service delivery.19 22 23 59 64 Coloniality, through the legacies imprinted in both postcolonial governance and health systems, continues to produce ripple effects in local implementation efforts. For instance, Wallace et al note that efforts to deliver reproductive healthcare in Timor-Leste are complicated by remnants of Portuguese colonisation in the form of Catholic values and haunting memories of Indonesia’s coercive and restrictive population control policies, both of which ‘shape availability and access to reproductive health services’ as well as the acceptability of those services to communities.21
Global health is undeniably shaped by the broader sociopolitical environment within which it operates, including the impacts of colonial values on legal and health systems that postcolonial countries continue to grapple with.44 Furthermore, the international nature of global health means that considerations of the contemporary political economy must extend beyond national borders, practically demonstrated by the way in which the Global Gag Rule (GGR) impacts the funding, service implementation and agency of organisations in receipt of US global health assistance during Republican administrations. As observed by Lane, Ayeb-Karlsson and Shahvisi, the GGR not only imposes restrictions on grant recipients and beneficiaries in the USA but also ‘on women living in global South countries, who have no input or involvement in the elections or policies of the U.S.’,22 and often with disproportionate effects on the most vulnerable and marginalised communities such as sex workers, men who have sex with men and transgender people.
A decolonial gender analysis can inform action for change
While the impacts of colonialism and coloniality on global health are well documented, seven papers20 33 35 48 50 66 69 in our study explored how a decolonial gender analysis could improve health outcomes and increase health equity. As Singh et al eloquently implore, we must move ‘beyond the performative dimensions of being gender-sensitive and decolonial, towards understanding what it means to equitably share power… in a meaningful way that challenges traditional methods’ and be explicit in considering how ‘gender intersects with other axes of power’.33
In this vein, this subset of seven papers called for changes in where we look for expertise and leadership, with an emphasis on ‘intersectional black, woman and feminist movements’20 69 and approaches developed across the global South,50 changes in the knowledge that we refer to with respect to underlying epistemological stance20 35 and the generation of ‘new’ knowledge,33 50 and a reconfiguration of how individuals and organisations work together.33 48 50 69
While significant changes are required at both the individual and structural levels, these papers highlight that there is no need to reinvent the wheel; there are strong traditions of praxis available to draw on, from both within and beyond global health35 48 (see also the work of Tuhiwai Smith73). However, we must acknowledge that any attempt to shift power will be perceived as a challenge to conventional bodies of authority20 and that there will be a need to provide, and perhaps reimagine, ‘safe spaces’ as is being advocated for within a range of activist spheres.48
Only when we have ‘safe spaces’ in which a cross-section of stakeholders and actors can come together through collective action will we be able to work on much-needed structural reforms, including: challenging the dominance of a narrative that ‘others’ and disempowers those that are ‘consistently categorised as vulnerable and needing protection or rescuing, which takes away their agency and power of action’;33 ‘dismantling barriers to healthcare by groups oppressed under colonial regimes’66 encompassing political, legal, ethical and cultural norms; and addressing how the next generation of (global) health professionals are educated.20 66
Taken as a set, these four themes tell a story about the ways in which intersecting colonial constructs of race and gender continue to drive contemporary inequities, how these constructs about individual and collective value and legitimacy bleed into modern notions of knowledge, how these forces continue to affect the implementation of health programmes and policies and, finally, how a decolonial gender analysis can inform action for change.
Conclusion: a call to integrate a decolonial gender analysis in global health and allied movements
This review identifies gender as a frequently overlooked dimension of decolonial discourses in global health, which is incommensurate with the role gender played in the colonial project and the influence that the coloniality of gender continues to have. While there has been a noticeable increase in discourse, with 93% (n=156/167) of the papers in our decolonising global health dataset published in the last 6 years, less than a third (n=53) had any reference to gender and only 16% (n=26) explicitly engaged with the intersection of gender and coloniality. As these 26 papers demonstrate, historical legacies of colonisation continue to shape racialised and gendered ideas about who is worthy (or not), limit the imagination of what programmes or interventions may be needed and affect what is possible to implement today.
We call for the integration of a decolonial gender analysis in approaches to decolonise global health research and programmes, acknowledging and confronting the multiheaded beast that is coloniality in its totality so that we do not risk allowing some forms of inequity to flourish unchecked while we confront others. This requires the recognition of the inextricable linkages between historical colonial constructs and contemporary gender inequalities and the use of intersectional feminist principles to interrogate and challenge power imbalances rooted in the coloniality of gender. Accompanying this call, however, are also words of caution. First, we reiterate Somerville and Munguambe’s warning to avoid using constructs of gender that are colonial in origin as our analytical starting point. Failure to do so would not only risk perpetuating a limited and limiting understanding of gender but also serve as ammunition for those who seek to deride and dismiss all efforts towards gender equality as a vehicle to impose ‘Western ideals’ on the rest of the world.36 At the same time, those working within global health must resist the urge to present a simplistic view which demonises all Western methodologies while reifying non-Western ways of knowing unquestioningly. Finally, it is crucial to remember that gender and decoloniality are just two of the many lenses that individuals and institutions are attempting to integrate,69 and this process must be carefully navigated to avoid ‘lens fatigue’.71
Drawing on the findings of this analysis, we also call for broader social justice movements to more explicitly integrate a decolonial gender analysis in applications of intersectional feminist approaches which identify, examine and challenge the roots of power asymmetries. Decolonial thinking draws clear lines between the past and the present, allowing those who incorporate it to treat not only the symptoms of contemporary power asymmetries but to confront the historical causes which remain embedded in systems and structures. These systems and structures work in tandem to ensure the continued exploitation and oppression of various communities and populations, necessitating initiatives and movements for justice and equality to also work together in confronting the many faces and forms of power. We call for an alliance of movements to address the shared colonial roots of racism, sexism, classism, ableism and other markers of marginalisation, breaking free from the yoke of shared oppression to find shared strength instead.
To that end, we offer three recommendations:
-
Movements advocating for the decolonisation of global health must integrate a gender lens and feminist perspectives into their analyses and actions if their aim is to uncover and dislodge the myriad manifestations of colonial influences on global health. Failing to do so will limit movements to partial and temporary success.
-
Opportunities for alliances must be identified and acted on. Power imbalances lie at the heart of all inequities; we must work with and not against each other to confront the primary cause of our shared struggles. In the absence of allyship, we leave space for mistrust and rivalry to fester in this time of increasingly limited resources for justice-centred movements.
-
Our answers to coloniality must not be neocolonial in design and implementation. Both within global health and among allied movements, we must ensure that the voices of the oppressed shape our agendas, approaches and actions. In short, we must ensure that decolonising movements are not themselves colonised74 or sanitised.
The manifestations of power asymmetries and other ongoing impacts of coloniality presented in this analysis are not exclusive to global health, providing an opportunity for global health actors intent on effecting change to learn from and share with other sectors. Thus, in closing, we stress once more the need for the integration of a gender analysis and feminist perspective into decolonial discourses, the prioritisation of collective action and alliances both within and beyond global health, and a constant process of reflexivity75 to ensure that we do not perpetuate that which we seek to dismantle. Ultimately, we argue that coloniality remains one of the root causes69 of many of the symptoms of our ailing world—confronting it requires a shift from focusing on competing goals to advancing shared visions for change.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We’d like to thank Dr Pascale Allotey, former Director of UNU-IIGH, for her critical input during the initiation of the decolonising global health work at the institute and for continually pushing us to consider the gender aspects. We’d also like to thank the many UNU-IIGH colleagues both past and present, with whom we’ve explored and discussed these ideas. In particular, we would like to thank Dr Johanna Riha for her extensive feedback on earlier versions of this manuscript, Dr Rifqah Roomaney who contributed to the larger dataset of which this analysis forms a part and Mr Rajat Khosla, Director of UNU-IIGH, and Dr Sagri Singh, Chief of Gender and Health, for their feedback and guidance. Finally, we extend our thanks to an anonymous reviewer for feedback on an earlier version of this manuscript.
[ad_2]
Source link
Northern areas attract thousands on Eid vacations

[ad_1]
ABBOTTABAD/
BALAKOT:
Packed with the baggage of cooked food, fruits and tents for camping at the picturesque Thandyani, Qaiser Khan and his family rejoiced after visiting their dream tourist resort during the Eidul Fitr holidays.
They enjoyed snow games, mountaineering and trekking amid rainy weather conditions.
An ex-Wapda employee, Qaisar and his sons Zershan and Ehtisham, enjoyed national and cultural songs such as “Sohni Dharti” and “Monga da Khyber Zalmi” on their music system. They were also busy fixing and hammering bolts on tents in a suitable location in Thandyani.
The family was looking forward to enjoying the rainy weather on the weekend without any cost. Amid disappearing sun behind clouds hovering over Thandyani hills amid blossom of seasonal flowers, Qaiser’s wife who belonged to Wapda Town Nowshera, was seen preparing green tea on a gas stove after warming up the Peshawar’s famous Chappli Kabab, Paye and Polao (rice dish) they brought along and making it ready on ‘Dastarkhwan’ to serve her family members on Saturday.
“Galiyat is my favourite tourist place. I planned Galiyat’s tour a few years ago but postponed it due to travel restrictions owing to the COVID-19 pandemic and today dream of my family to see its mesmerising natural beauty with soothing environment came true,” said Qaiser.
Wearing traditional Peshawari Chappal, the 59-year-old tourist said that he had brought tents and other stuff along as the hotel room and food cost is very high for a common man at Galiyat. “The rent of a normal two-bedroom per night in Thandyani and Nathiyagali is approximately Rs10,000 to Rs12,000 which was beyond the capacity of the middle class”, he added.
Like Qaiser Khan, thousands of families and tourists arrived at northern Khyber Pakthunkhwa especially Malakand and Hazara divisions including Galiyat and Thandyani to explore its waterfalls, gushing rivers and lakes of Saiful Malook, Ansoo, Dudipath and Mahoodhand and colonial era tracks besides enjoying the expensive trout fish and water boating in River Kunhar at Kaghan and Khanpur dam at Haripur.
“Despite torrential rains in K-P and Punjab, the response of tourists, adventurers and sportsmen in Malakand and Hazara during the Eid holidays was impressive,” Saad Khan, said the spokesman for the Cultural and Tourism Authority.\
He said that Galiyat, Thandyani and Nathiagali, Kaghan and Naran including Saiful Malook and Ansoo lakes in Manshera district were the most visited destinations during the Eid holidays.
Four Integrated Tourism Zones (ITZ) would be developed at Mankiyal Swat, Thandyani Abbottabad, Ganol Manshera and Madaklasht Lower Chitral, Khan said, adding these ITZs would be constructed with a loan grant of $70 million from the World Bank. He further said that the ITZs of Thandyani and Mankiyal would be connected with Swat and Hazara motorways through link roads that would open up entire Malakand and Hazara for tourists and make Pakistan a hub of international tourism.
Published in The Express Tribune, April 14th, 2024.
[ad_2]
Source link
AI model has potential to detect risk of childbirth-related post-traumatic stress disorder

[ad_1]
Researchers have adapted an artificial intelligence (AI) program to identify signs of childbirth-related post-traumatic stress disorder (CB-PTSD) by evaluating short narrative statements of patients who have given birth. The program successfully identified a large proportion of participants likely to have the disorder, and with further refinements—such as details from medical records and birth experience data from diverse populations—the model could potentially identify a large percentage of those at risk. The study, which was funded by the National Institutes of Health, appears in Scientific Reports.
Worldwide, CB-PTSD affects about 8 million people who give birth each year, and current practice for diagnosing CB-PTSD requires a physician evaluation, which is time-consuming and costly. An effective screening method has the potential to rapidly and inexpensively identify large numbers of postpartum patients who could benefit from diagnosis and treatment. Untreated CB-PTSD may interfere with breastfeeding, bonding with the infant and the desire for a future pregnancy. It also may worsen maternal depression, which can lead to suicidal thoughts and behaviors.
Investigators administered the CB-PTSD Checklist, which is a questionnaire designed to screen for the disorder, to 1,295 postpartum people. Participants also provided short narratives of approximately 30 words about their childbirth experience. Researchers then trained an AI model to analyze a subset of narratives from patients who also tested high for CB-PTSD symptoms on the questionnaire. Next, the model was used to analyze a different subset of narratives for evidence of CB-PTSD. Overall, the model correctly identified the narratives of participants who were likely to have CB-PTSD because they scored high on the questionnaire.
The authors believe their work could eventually make the diagnosis of childbirth post-traumatic stress disorder more accessible, providing a means to compensate for past socioeconomic, racial, and ethnic disparities.
The study was conducted by Alon Bartal, Ph.D., of Bar Ilan University in Israel, and led by senior author Sharon Dekel, Ph.D., of Massachusetts General Hospital and Harvard Medical School, Boston. Funding was provided by NIH’s Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
Source: NIH
[ad_2]
Source link
Call for action: addressing the alarming surge of HIV in Madagascar
[ad_1]
Summary box
-
In Madagascar, the HIV epidemic was long thought to be concentrated on key populations like sex workers, men who have sex with men and intravenous drug users. Although weaknesses in the national epidemiological HIV surveillance have been described, mounting evidence now reveals a surge in HIV across populations and regions, indicating a potential transition of the epidemic to vulnerable and the general population.
-
Despite broadening its national HIV strategy, the lack of larger epidemiological studies hampers international support and consequently the country’s ability for a comprehensive response, leading to inadequate HIV awareness, care services and research initiatives.
-
The authors, representing academic, civil society and governmental sectors involved in the HIV response, urge immediate collaborative action between national and international stakeholders to expand HIV interventions, bridge funding gaps and deepen epidemiological understanding for a more robust national HIV response.
In stark contrast to its neighbours in Sub-Saharan Africa, Madagascar reports an estimated HIV prevalence below 0.5%.1 HIV infections are perceived to be primarily concentrated in key populations. However, closer inspection suggests an underestimated epidemic transitioning to the general population.
A 2020 analysis by Raberahona et al on the status of HIV in Madagascar already suggested that the country may be on the verge of a high-prevalence epidemic, with a concerning rise in sexually transmitted infections (STIs) in the general population, elevated HIV rates among sex workers and an increase in cases newly diagnosed with late-stage disease.2 The study also underscores weaknesses in the epidemiological surveillance of HIV.
A recent study in a high-risk region reports an unprecedented 2.9% HIV prevalence in the general population, soaring to 13% in urban areas.3 Experts from various regions report a continuing surge in HIV positivity rates and AIDS-defining conditions, with many patients unaware of their serological status. Obstetricians observed a 7% HIV prevalence in pregnant women in a northern district in 2023, with limited testing and treatment capacities leading to untreated pregnant women and newborns being born without prophylaxis or treatment (C. Benski, unpublished). Hospital cohort data show a rise in newly diagnosed HIV cases during admission, increasing from 0% to 25.4% between 2010 and 2016, and patients diagnosed in stage 3 and/or 4 rose from 6.6% to 38.9%.4 An increase in extrapulmonary tuberculosis (TB) cases, mainly lymphadenopathy, revealed by TB surveillance data, raises further concern. Limited diagnostic resources frequently necessitate reliance on clinical assessment for diagnosis, hindering the exclusion of differentials. In a study assessing the specificity and sensitivity of molecular diagnostics for extrapulmonary TB, Rakotoarivelo et al found a 12% HIV positivity rate among clinically diagnosed cases, hinting at a potential connection with the HIV epidemic.5
Madagascar’s population faces heightened vulnerability to STI transmission. A 2018 demographic survey reveals 18%–20% of individuals aged 15–49 having multiple concurrent sexual partners, with low condom usage (less than 5% among those aged 15–24).6 A 2021 health survey shows less than 27% have a comprehensive understanding of HIV transmission, and three out of four exhibit stigmata towards people living with HIV. The majority (82%–92%) has never undergone an HIV test, and only 3% of women are aware of their serological status.7 A cross-sectional study on STI prevention among university students indicates over one in three engage in high-risk sexual behaviour.8 Madagascar’s artisanal mining sector, exceeding one million in 2014, poses additional transmission risks with its young population, frequent migration, transactional sex driven by local economic factors and limited healthcare access within a highly informal sector, further amplifying risks and vulnerabilities.9
According to the World Bank, eight of 10 people in Madagascar live in monetary poverty (with a daily consumption below USD 2.15 per person).10 With 1.9 medical doctors and 2.9 nurses and midwives per 10 000 in 2019, Madagascar’s health worker density is particularly low.11
A recent modelling study, considering these contextual factors, forecasts a transition to a generalised HIV epidemic with a prevalence rate of 9%–24% in the general population within the next decade unless testing and treatment efforts are escalated.12
In Madagascar’s population of 28.9 million, UNAIDS estimates 70 000 HIV cases in 2022, with 18% of cases receiving antiretroviral treatment.1 The country recently expanded its national HIV strategy to move beyond key populations, including vulnerable groups like the youth and individuals with STIs, and bridge populations. However, the Global Fund, the primary funder of the country’s HIV response, constrains its funding to target key populations in hot spot cities, resulting in insufficient testing capacities for vulnerable groups. This includes shortages of rapid tests and trained healthcare workers for HIV counselling and care across sectors and levels. Despite repeated appeals for increased funding to implement the national HIV strategy, the international response has been limited. International funders withhold additional resources in the absence of robust evidence, leaving local stakeholders unable to generate the necessary proof—a vicious circle of delayed awareness and response.
Given Madagascar’s healthcare system and the population’s vulnerability, this urgent plea implores national and international organisations and funding bodies to address this health crisis. We strongly advocate for expanding funding to ensure comprehensive HIV awareness, prevention, diagnostics, medical treatment and psychosocial support, encompassing not only key populations but also vulnerable and bridge populations. Strengthening research initiatives is imperative to fill gaps in epidemiological, sociocultural and implementation knowledge, providing a crucial foundation for a resilient public health response to Madagascar’s escalating HIV epidemic.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
[ad_2]
Source link
Meta’s WhatsApp down for thousands, Downdetector shows

[ad_1]
Meta Platforms-owned (META.O) WhatsApp was down for thousands of users on Wednesday, according to outage tracking website Downdetector.com.
There were about 12,000 incidents of US users reporting issues with the messaging platform, according to Downdetector, which tracks outages by collating status reports from a number of sources including user-submitted errors on its platform.
More than 20,000 users in India, about 46,000 in the United Kingdom and over 42,000 in Brazil have also reported problems with the platform, Downdetector data showed.
Read more: WhatsApp to let you pin up to three messages in chats
Around 4,800 people also faced issues with Instagram in the United States, according to Downdetector.
Meta did not immediately respond to a Reuters request for comment.
Last month, hundreds of thousands of users of the social media company’s Facebook and Instagram globally were impacted for more than two hours following an outage that was caused by a technical issue.
[ad_2]
Source link
Aligning the principles and practice of research integrity and research fairness in global health: a mixed-methods study
[ad_1]
WHAT IS ALREADY KNOWN ON THIS TOPIC
-
Over the past decade, the ideals of research integrity and research fairness have gained considerable momentum in global health. While both have been the subject of intense academic debate, there is little empirical data on actual practices related to integrity and fairness specific to global health.
WHAT THIS STUDY ADDS
-
Findings suggest that global health researchers mostly adhere to research integrity and research fairness principles. Some behaviours are more frequently reported (transparent reporting of studies, seeking local ethical approval) than others (engagement with affected populations, engagement with local decision-makers, adherence to Open Science), with little variation between responses from the Global North and the Global South.
-
We identified several structural, institutional and individual factors associated with these patterns, such as an inflexible donor landscape, research institutions’ investments in relationship building, guidelines and mentoring, as well as power differentials and competition between researchers.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
-
This study shows there are more synergies than trade-offs between research integrity and fairness as they share similar determinants and the same goal of increasing research quality and maximising the societal benefits of research. There is ample scope to make such synergies explicit and to align both agendas in global health.
Introduction
Global health decisions are often made remotely, without consideration for the people they affect.1 Ideally, the conduct of global health research should straddle the twin ideals of research integrity and research fairness2 and should follow practices that guarantee the validity and trustworthiness of science.3 It should also aim to transcend the ‘distance’ between research teams and researched populations that currently characterises the study of global health problems. While the pursuit of integrity and fairness in global health can conflict ideologically,4 they share the same goal of increasing the societal benefits of research. Addressing these breaches of research integrity and fairness requires an understanding of the magnitude of the problem and its determinants.
Over the past decade, research integrity and research fairness have gained considerable momentum globally. Research integrity emerged in the late 2000s as a response to the reproducibility crisis in science.5 It encompasses all professional codes promoting Responsible Research Practices (RRPs), with a strong traditional focus on individual researchers’ responsibilities,6 but increasingly recognising the role of research environments in shaping collaborations3 7 and reward systems.8 9 Research integrity is closely intertwined with Open Science, which promotes full transparency of research processes to maximise reproducibility.10 Research fairness,11 on the other hand, encompasses a broad range of initiatives from the mid-2010s to promote fair and equitable research partnerships12 13 and a holistic understanding of global challenges. Research fairness initiatives aim to increase ownership of research agendas and outputs in Low-income and Middle-Income Countries (LMICs), thereby maximising the positive impact on local research systems and populations. These initiatives focus on power imbalances between actors in previously colonising and colonised nations and as such are broadly aligned with recent calls to ‘decolonise global health’.14 Research integrity and research fairness share the goal of increasing research quality and maximising the societal benefits of research by following two different paths.4 While research integrity prioritises, rewards and reinforces scientific processes in the pursuit of global and generalisable knowledge, research fairness is geared towards local information needs and favours knowledge production that reflects the ‘lived experience of people themselves’.14
Research integrity has been the subject of many scholarly debates, and recent surveys have reported the prevalence of Questionable Research practices (QRPs).15 16 QRPs are defined as ‘subtle trespasses’15 or ‘misbehaviours’17 that lie in the grey zone between fabrication, falsification and plagiarism on one side, and responsible research conduct on the other. The term includes practices such as not reporting flaws in study design or execution, selective citation to enhance one’s findings and so forth.15 It is sometimes argued that the ‘prevention paradox’ applies to research integrity—while QRPs may constitute a less severe offence compared with fabrication and falsification their frequency makes them more damaging to science.18 This is backed up by data: estimates of data fabrication or falsification from a recent study in the Netherlands were just above 4%15 while over 50% of researchers engaged frequently in at least one QRP. This is in line with a Nature study that revealed that ‘more than 50% of researchers are unable to reproduce their own work’.5 There are no data specifically for global health research, however, there is no reason to believe that it fares better than other types of research.19
Research fairness has also been the subject of academic scrutiny, with substantial evidence that the current global health research ecosystem is unfairly skewed towards institutions and scientists in High-Income Countries (HICs). A systematic review found that 28% of studies mentioned some kind of ‘discriminatory power imbalance’ between Global North and South research team members.1 Studies have shown that LMIC research agendas are led by donors in HICs,20 with research funding disproportionately allocated to HIC institutes.21 To our knowledge, there are no systematic analyses of global health research funding flows, but donor reports and tracking tools reveal that approximately 70% of funding is channelled through Global North institution.20 22–26 Studies on roles and perceptions of researchers in global health collaborations show that local researchers are often relegated as ‘glorified field workers’27 with no influence on study design28 and less likely to be in prominent author positions.29
While research integrity and fairness are both intensely researched, no studies to date have investigated research practices jointly influencing integrity and fairness in global health. Therefore, little is known about potential synergies and trade-offs. For example, are efforts to increase research integrity improving research fairness and vice versa? Or are strategies to increase one affecting researchers’ ability to improve on the other? Furthermore, we do not know whether there are fundamentally diverse ways of conducting research in different areas of the world, more specifically between those who are conducting research from ‘afar’ (eg, researchers based in the Global North conducting research in the Global South) versus those conducting research nearby (ie, Global South researchers conducting research in their settings). Furthermore, the research integrity agenda has so far been dominated by Global North actors, which could potentially lead to different levels of adherence to research integrity principles across geographies.
Limited research on both research integrity and fairness in global health means there is little data to support either debate—beyond norms or guidelines. Yet data on desired and undesired practices, barriers and facilitators, can provide evidence to develop improvement strategies and baselines to measure progress. To provide this information, we conducted a mixed-methods study to estimate the frequency and to explore the determinants of practices associated with research integrity and research fairness.
Methods
This mixed-methods research study combined an online survey (quantitative component) with online in-depth key informant interviews (qualitative component). The quantitative component estimated the frequency of research practices by measuring self-reported adherence to norms and guidelines of research integrity and fairness. The qualitative component aimed to provide context and to explore determinants, that is, barriers and facilitators for such practices. Determinants could be described at individual (concerning the researchers themselves), institutional (regarding academic institutes) and structural (the wider research landscape) levels. The qualitative research tools were based on preliminary analyses of the quantitative component (exploratory approach). In line with previous research integrity surveys, we defined QRPs as ‘misbehaviours (that) lie somewhere on a continuum between scientific fraud, bias and simple carelessness’.17 Following this logic, we defined Unfair Research Practices (URPs) as behaviours that perpetuate power imbalances, marginalisation, exploitation and inequality in the production and dissemination of knowledge. As opposed to QRPs and URPs, RRPs and Fair Research Practices (FRPs) promote positive behaviours related to research integrity and fairness respectively. This study builds on a pre-existing pilot study.30
Data collection tools
The questionnaire for the online survey can be found in the repository. This self-administered survey was developed and emailed to researchers in English. This tool lists 20 QRP/RRPs related to research integrity and 20 URP/FRPs related to research fairness, including adaptations of questions developed by the Dutch National Survey on Research Integrity (NSRI)31 that are in line with the Bridging Research Integrityamd Global Health Epidemiology (BRIDGE) criteria.4 Alignment with the NSRI was done to enable comparisons and because the NSRI questions underwent prior psychometric validation.4 15 For research fairness, we developed 20 URP/FRPs derived from the BRIDGE criteria. Like the NSRI survey we used statements in the first person, a 3-year recall period and a 7-point Likert scale to retain similar levels of content and construct validity. The Likert scale consisted of the following values: 1=never, 2=very rarely, 3=rarely, 4=occasionally, 5=frequently, 6=very frequently and 7=always. To avoid straight lining, some statements were phrased as a questionable/unfair and some as responsible/fair.
The in-depth interview schedule was based on the BRIDGE guidelines and included topics on participants’ experiences with QRPs and URPs and determinants of these practices. This schedule covered all six phases of an epidemiological study (preparation, protocol development, data collection, data management, data analysis and reporting). The interviewers navigated the conversations according to interviewees’ preferences for focusing on given study phases and exploring contributing factors. Interviewers probed interviewees for statements where quantitative findings showed the strongest differences or overall lowest or highest scores. We aimed at receiving maximum variation of phases among interviews. All interviews were conducted in English.
Study population and setting
The study population consisted of researchers currently involved in global health and working in institutes that are part of the following networks: tropED (Network for Education in International Health), INDEPTH Network, Asian Health and Demographic Surveillance System Network, Astra South Asia, African Institute of Mathematical Science, Consortium of Universities for Global Health, Humanitarian Health Ethics Network, Collaboration for Evidence Based Health Care in Africa, Trials of Excellence in Southern Africa, West African and Central African Network for TB, HIV/AIDS and Malaria, East African Consortium for Clinical Sciences, Bill & Melinda Gates Foundation Global Health Grantees, Southeast Asia One Health University Network, COVID-19 Clinical Research Coalition and the European and Developing Countries Trial Partnership. We used the algorithm in figure 1 to assess eligibility of institutions within the sample framework. ‘Relevant institutions’ included universities, non-profit non-government research/knowledge centres, government research institutes or funding institutions with a role in research development. ‘Relevant type of research’ included global health (international) or public health (national) research involving interactions with communities, patients, public or other local actors (ie, not laboratory or document based).

Algorithm to assess the eligibility of institutions.
Institutes were categorised by geographical location—Global North and Global South—to enable stratified sampling and equal geographical distribution of institutes across geographies. In the absence of an objective measurement to classify countries as Global North or South, we referred to the World Bank 2021 country income classifications32 in LMICs, upper-middle-income countries (UMICs) and HICs. More specifically, LMICs and UMICs were considered as Global South, and HICs as Global North. During quantitative data collection, participants were asked to self-identify as either Global North or Global South, with possibilities including ‘prefer not to disclose’ or ‘other’. In-depth interviews revealed that this category includes researchers raised, trained or working in different countries across north/south divide and reclassified as Global Neutral.
Sampling and sample size
For the online survey, participants were sampled using two-stage stratified cluster sampling. The sample size was calculated based on a Z-score of 1.96, a hypothesised prevalence of 50% for QRP/URPs, a precision of 10% on each side of the prevalence estimate, a design effect of 3, a 50% response rate and an additional 10% institutional attrition rate. Overall, the estimated (target) sample size per stratum was rounded up to 900. This sample was achieved by randomly selecting 30 institutes per stratum and 30 individuals per institute, in the first sampling stage. In the second stage, we compiled lists of all researchers listed on publicly available websites working in the selected institutes. Researchers were randomly selected from the compiled list and invited to participate in the online survey.
During the online survey, we captured participants’ willingness to participate in the in-depth interview. We invited three to four willing participants per strata to participate in interviews making a total of nine interviewees and we reached saturation with this sample size. Although we initially planned to select Global North and Global South researchers equally, two participants identified as ‘Global Neutral’ during the interview.
Data analyses
The frequency survey had two main outcome variables: (1) RRP score and (2) FRP score. Since the questionnaire provided statements phrased either as questionable/unfair practice or as responsible/fair, we recoded responses to align all responses on a positive scale, whereby a score of “1” for RRP or FRP denoted never engaging in that practice and a score of “7” denoted very frequent engagement. In other words, high scores for both the RRP and FRP score denoted desirable behaviours from an integrity and fairness standpoint.
We then grouped the RRP and FRP questions into behaviour domains (online supplemental table 1). RRPs questions were grouped under (1) following meticulous research process; (2) mentoring of junior researchers, (3) ensuring adequate methods; (4) aiming for transparent reporting; (5) striving for reproducibility and (6) engaging with open science. FRPs were grouped under (1) aiming for engagement of local decision-makers; (2) aiming for engagement of affected populations; (3) working in partnership with local researchers; (4) striving for fair agreements between study partners; (5) seeking local ethical approval and (6) ensuring respectful data collection.
We reported the median (and IQR) of Likert scale responses for each RRP and FRP. Average scores in each behaviour domain were derived followed by median and IQRs. This two-step process involved estimating a mean score for each behaviour domain and estimating the overall mean for each domain. Statistical differences between the Global North and Global South researchers for individual practices (RRP and FRP) were explored using the Wilcoxon rank sum test and differences across each of the 12 domains were with a Student’s t-test. We used linear regression to explore individual factors associated with RRPs and FRPs. We included the researcher’s age, gender, seniority (highest attained degree), discipline of the researcher, place of origin (Global South researcher working for Global North institutions or vice versa), years of involvement in research and role of the researcher as independent variables. We reported the results as adjusted coefficient, 95% CI and p values.
For the qualitative analyses, we used the six phases of the BRIDGE guidelines to create codes (deductive approach) and later added new codes arising from the data (inductive approach). Relevant and similar codes were merged into categories and analysed to identify themes arising from the data. We used NVivo software V.11 for data coding and analysis.
Data management
We used Survey Monkey to collect quantitative data online adhering to global data safety and protection practices like limiting identifiable researcher information and automatically deleting stored data after 13 months. Participants provided some indirect identifiers during the data collection, including geographical region of institute and level of experience, to prospectively strengthen the analysis and allow us to explore the data in different strata. These data, however, were presented carefully to prevent the identification of individual members.
Qualitative data collected were audio recorded in online meeting platforms, following informed consent and anonymised prior to storing in a password-protected online folder. The qualitative data from the interviews were transcribed using otter.ai and were checked and edited manually for all the transcripts. Personal identifiers were removed throughout the transcription and coding processes and labelled based on their identification as Global North (GN), Global South (GS) or Global Neutral (GX) researchers.
Patient and public involvement
This meta-research study is not conducted on patients but on researchers themselves. Researchers were consulted in the past with a Delphi study for the development of the BRIDGE guidelines that laid the foundations of this research. In addition, we set up a study task force including researchers from South Africa, India and the Netherlands that independently reviewed this study’s tools and methods ahead of data collection. This publication will be shared with all researchers who participated in this study.
Results
Sample description
Of the 1717 researchers contacted to participate in the survey, 145 (8.4% responded). Response rates were slightly higher for researchers in the Global South than the Global North at 9.5% (n=82) and 6.2% (n=53), respectively.
The survey participants’ country of origin exhibited a geographical distribution, with India comprising 9.0% (n=13) of respondents, followed by South Africa, Switzerland and the UK, each accounting for 5.5% (n=8). The USA constituted 4.8% (n=7) and represented a significant portion of respondents. Additionally, researchers from Nigeria (n=6), Ghana (n=5), Belgium, Germany, Zambia and Portugal, each contributing three respondents, were identified. Furthermore, Kenya, the Philippines, Uganda and Australia (n=2) were represented, while Bangladesh, Indonesia, Ivory Coast, Malaysia, Sudan and Vietnam each had one participant. While 44% (n=64) either did not respond to the question or preferred not to disclose the geographical location of their country of origin.
Professional and demographic details of survey participants can be found in table 1, though this information was provided by at most 118 (81.4%) of the researchers. Overall, our sample is slightly skewed towards Global South researchers (56.6%). The relative majority of participants were based in sub-Saharan Africa (28.3%), closely followed by those in Europe and Central Asia (22.1%).
Professional demographics of the researchers
In terms of disciplinary background, most researchers had a biomedical background with the highest number of researchers reporting biostatistics/epidemiology as their discipline (29.0%) or biology/medicine (22.8%). Men and women are approximately equally distributed (40.7% vs 38.6%) although interestingly global south researchers were slightly more likely to be men and global north researchers slightly more likely to be women. In terms of seniority, our sample was skewed towards senior researchers with the largest group of researchers (44.8%) being established researchers with more than 10 years posteducation, followed by mid-career researchers with 3–10 years posteducation (24.8%). Most researchers had up to a PhD degree (23.4%) or were university professors (22.8%).
Research integrity and fairness behaviour domains
An analysis of frequency scores, by location (Global North vs Global South) and research behaviour domains (online supplemental table 1), shows some variation between domains but little by geographical location. These are summarised in figure 2 with further details in online supplemental table 2. Participants based in the Global South had statistically significantly higher mean scores of mentoring compared with the Global North (5.72 (SD: 1.03) vs 6.15 (1.32)) (p=0.001) as well as engagement of affected populations (4.44 (SD: 1.35) vs 5.08 (SD: 1.71) (p=0.038). We defined good mentoring as sufficiently supervising junior coworkers and giving sufficient attention to the skills or expertise to perform studies. While the engagement of affected populations comprised questions on consulting representatives of affected populations during the preparation stage of research or to develop lay dissemination products and developing dissemination products specifically for affected populations or their representatives. The highest frequency score overall was for seeking local ethical approval (online supplemental table 2) at 6.62 (SD=1.09). On the other hand, four domains stand out for having relatively lower scores around 5 (corresponding to frequently engaging in the behaviour): engagement of affected populations (consulting representatives of affected parties at preparation and dissemination, developing lay dissemination tools); engagement of local decision-makers (consulting end users at preparation phase and when developing lay dissemination material); open science (publishing articles and datasets open access) and ensuring reproducibility (preregistering study protocols, publishing valid negative studies, taking steps to correct errors in published work) (figure 2 and online supplemental table 2).
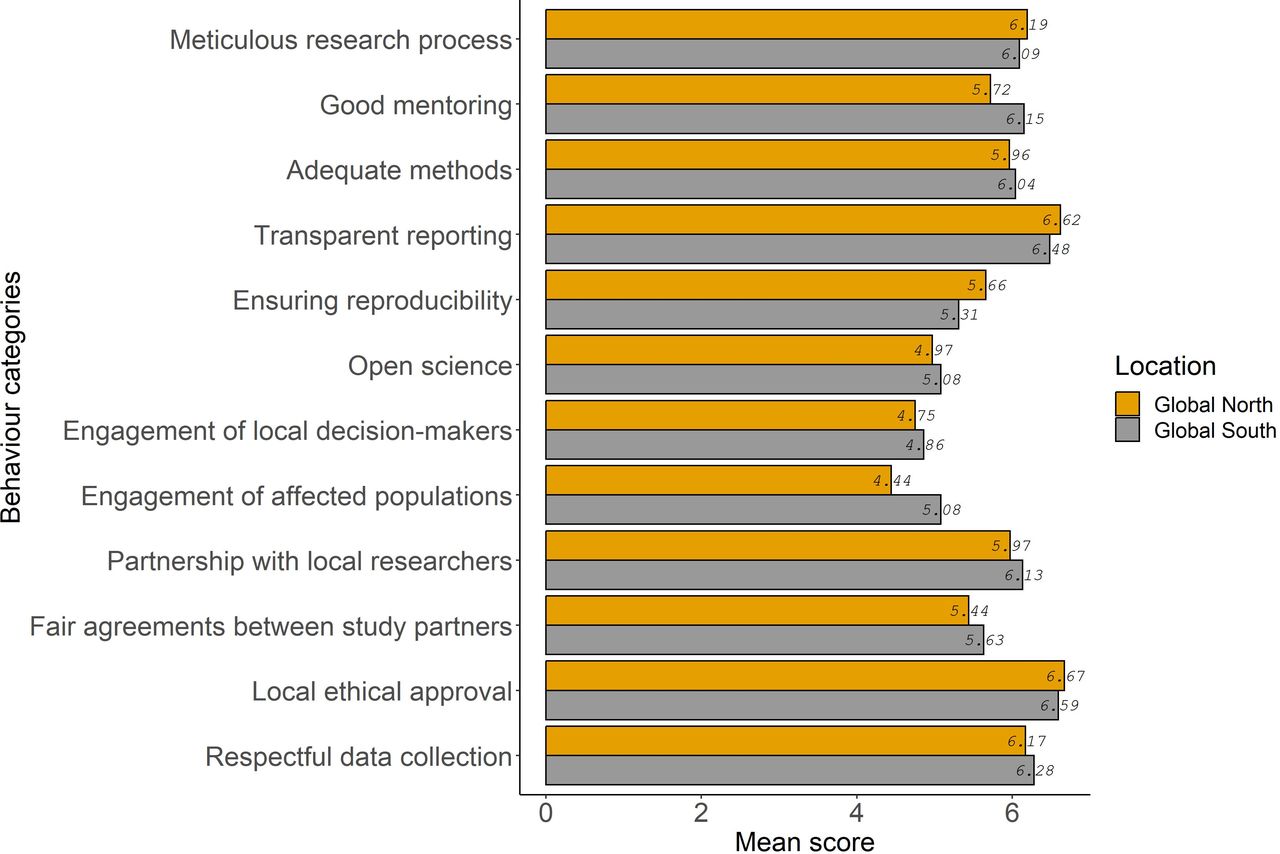
Research integrity and research fairness frequency scores, by domain and location of the researchers.
Differences in research practices between Global North and Global South researchers
Despite overall similar behaviour between Global North and Global South researchers, a detailed review of each individual practice reveals a consistent trend whereby researchers based in the Global South report more desirable behaviour, with small but significant differences across many subindicators. Median Likert scores for individual questions are presented overall and by location (Global North and Global South) in online supplemental table 3. Three main findings emerged about Global South researchers: (1) they are more likely to report having the skills and expertise essential to perform studies and sufficient supervision or mentoring of junior coworkers; (2) more likely to report consulting representatives of affected populations and end-users and (3) more likely to report having clear decision-making processes, using data sharing agreements (but less likely to report the strategies put in place to encourage data reanalysis by local researchers).
First, there are differences regarding enough attention to skills and expertise necessary and sufficient mentoring of junior coworkers, Global South researchers reported a median score of 7 (corresponding to ‘always’ as per the Likert scale) whereas Global North researchers reported a median score of 6 (very frequently). The in-depth interviews provide some context to make sense of these differences. With regard to giving sufficient attention to skills or expertise, Global North as well as Global South interviewees discussed that Global North research institutes more frequently have a leadership role, even if they lack context-specific expertise and knowledge, which may explain the slightly lower scores reported by Global North researchers. Regarding sufficient mentoring and supervision of junior coworkers, some Global South participants referred to ‘helicopter research’ projects by Global North research, as projects that are frequently insufficiently overseen by far-away supervisors. Furthermore, one Global North researcher admitted that as a junior researcher, they found themselve not receiving sufficient mentoring and supervision on decision-making processes, when they were placed in a coordinating role of a research project in the Global South, suggesting that their junior rank did not meet the level of experience necessary for the role and responsibilities.
Second, with regard to consulting end-users of research and affected populations, differences were observed when participants were asked if they consulted representatives of affected populations during the preparation stage of research. There was a statistically significant difference in the median responses between Global South researchers who reported a score of 7 (corresponding to ‘always’ as per the Likert scale) and Global North with a score of 5 (frequently) (p<0.0001) (online supplemental table 3). There was also a statistically significant difference in researchers’ responses to whether they consulted end-users of the research during the preparation stage of the research between Global South’s median score of 6 (very frequently) and Global North with a median score of 5 (frequently) (p=0.032) (online supplemental table 3). Interestingly, most qualitative data for these aspects was discussed by the researchers based in the Global South, despite their higher scores. Most participants identified the need to communicate with the local communities before, during and after the research and indicated that project/funding timelines do not provide sufficient time to do it properly: ‘…Going back to the… the community itself is. Is not…is not something that that we are good at doing.’ [GS3].
Third, when asked whether the research they were involved in had clear and fair data ownership agreements, we found statistically significant differences between the Global South, median score of 7 (always), compared with the Global North, median score of 6 (very frequently) (p=0.045) (online supplemental table 3). This was a similar difference to the one found in the question of having clearly agreed decision-making processes. Furthermore, there was a statistically significant difference in the researchers’ responses to whether strategies were put in place to encourage secondary analyses by local researchers when data was made openly available. For Global South researchers, the median score was 6 (very frequently), and for the Global North, the median score was 4 (occasionally) (p=0.037) (online supplemental table 3). These results suggest that data-sharing agreements may do little to promote reanalyses by local researchers. The few interview responses on this topic confirmed that there is an issue with the misuse or re-use of data either in the absence of agreements or beyond the original intention of the study. They also described the increased use of data-sharing agreements over time and how these agreements are only part of the solution: preventing issues with data-sharing relies more on trust and confidence between partners.
Determinants of research integrity and fairness
The study of determinants of research integrity and fairness was done both qualitatively to study structural, institutional and individual determinants of research integrity; and quantitatively (with a regression model) to estimate the effect of individual determinants (association between professional characteristics on the overall research fairness and research integrity scores).
Structural determinants
Most interviewees addressed the inflexible and inequitable donor landscape, where funding streams largely flow from Global North donors to Global North institutes, who subsequently subcontract their partners in the Global South. This funding pattern reportedly reinforces a top-down structure to the research partnership with unequal power dynamics, roles and responsibilities between Global North and Global South researchers frequently defined from the onset of a collaboration. Another structural factor mentioned by several participants was time and resource pressure, especially during the proposal and protocol development phases. This limits the fair involvement of affected populations and end-users of research as well as the ability to cocreate study tools and jointly plan fieldwork. This limited involvement can also extend to members of the research team, where pressures on the partnership leads to delegated roles in research project. The most commonly reported example is the practice of subcontracting fieldwork or data collection to a Global South team who have limited insight or influence on the prior or later stages of the research. Some interviewees further stressed that the competition between research institutes in the acquisition of work in the global health arena further intensifies the pressure on both Global North and South institutes, which can encourage URPs and QRPs.
Another structural determinant that emerged strongly from the qualitative data concerns issues around trust in research partnerships and distinct skills and qualities ascribed to researchers that are rooted in colonialism and racism.
Sometimes they think that they are white girls, boys will do better, they know better than the south, than the brown skin or black skin, (…) that maybe (we) will not do our work properly, not produce the quality,(…). So there is also a negative (attitude), without any ground, without working with somebody, they have this mindset. (…) So there’s also this colonising mentality that black people, they are lazy. They don’t do their or they don’t have the quality we can trust them. They couldn’t manage. (GS4)
The pervasiveness of neocolonial sentiments was also recognised to transcend the Global North/South divide:
I don’t think that colonisation is something that belongs to (the) North. I think it’s a concept like patriarchy. And women can be as patriarchal as possible. It doesn’t have to be men. It’s a practice, it’s a belief…. there are a lot of Southern people around (who) are also in power in the northern global hemisphere. I don’t see them behave differently. (GS4)
When it comes to dissemination and communication of results, both Global North and South participants stated that necessary but unpaid hours needed to publish in peer-reviewed journals influenced the levels of fair coauthorship. Some participants also stated that the additional responsibilities of executing projects and moving from project to project does not allow them to prioritise publications. Some interviewees also shared accounts of concerns with personal finances and livelihood putting pressure on researchers. This can lead to QRPs, such as fabricating patients and pocketing their financial reimbursement. Lastly, some responses suggest that cultural factors can also influence research practices. A specific example given by a Global South researcher concerned the practice around informally tipping gatekeepers and study participants to incentivise participation which can be viewed as questionable.
Institutional determinants: Several interviewees considered the level of buy-in and commitment to fair and robust research practices by the senior leadership in academic institutions as a crucial factor. Related to this, a lack of training and reflexivity around ethics and relationship building was often discussed:
I think people aren’t trained in relationships. (…) I mean, what if, if that could really change, those relationships could be more open, and we could more openly reflect on them with each other too, I think you could see real change. But then you have to really value like, what does it mean to create and foster a partnership? And I don’t know any curriculum that’s doing that in global health. (GN3)
While most interviewees, based in the Global North and South, acknowledged insufficient institutional commitment to addressing URPs and QRPs, some participants perceived increasing investments in training and guideline development around ethics and fairness in Global North institutes. Some interviewees recognised, however, the different institutional dynamics at northern and southern institutes, with greater overheads in the Global North affording more institutional support for safeguarding research integrity. Time constraints can also be understood as an institutional factor affecting research fairness and integrity, which interviewees addressed in relation to delayed contracting and ethics review, which can hamper the meaningful involvement and fair treatment of southern partners. Further, as previously discussed, insufficient supervision of students or junior staff also emerged as an individual determinant negatively affecting research fairness and integrity.
Individual determinants
The regression models fitted to explore the association between research practices and demographic/professional characteristics of researchers do not support strong hypotheses regarding their effect of individual determinants (online supplemental tables 4 and 5). Indeed, while some Wald tests are significant, most overall log-likelihood ratio tests are not. The only independent individual determinant which emerged from the regression analysis (beyond Global North and Global South differences discussed above) was academic rank (with more senior rank reporting more desirable behaviour) and discipline of the researcher (with biomedical sciences reporting higher scores than medicine) after adjusting for other factors. Indeed, bachelors or masters level degree was associated with a −14.0 (95% CI –27.0 to –0.74) (Wald test p=0.042) reduction in the responsible research score compared with associate professor or full professor in multivariate analyses after adjusting for location, career length, gender, geographical region the researcher and discipline of the researcher of global health. Researchers from the biomedical science discipline were associated with a −43.0 (95% CI −71.0 to –16.0) (Wald test p=0.002) reduction in the responsible research score compared with biology/medicine in the multivariate analysis after adjusting for location, years of involvement, gender, geographical region the researcher’s institute and academic rank (online supplemental table 4). When it comes to FRPs, the only independent individual determinants emerging from the regression analysis were career length and discipline. Indeed, the environmental and occupational research discipline was associated with a 18.0 (95% CI 1.1 to 35.0) (Wald test p=0.004) increase in the fair research score compared with biology/medicine in the multivariate analysis after adjusting for location, years of involvement, gender, geographical region the researcher’s institute and academic rank. Researchers preferring not to disclose their career length were associated with a −50.0 (95% CI -99 to −1.6) (Wald test p=0.046) reduction in the fair research score compared with Early Career (<3 years posteducation) in the multivariate analysis after adjusting for location, years of involvement, gender, geographical region the researcher’s institute and academic rank (online supplemental table 5). However, it is important to note that according to overall likelihood ratio tests for RRPs, the p value for the discipline of the researcher was significant (p=0.029) while for FRPs neither the academic rank nor the discipline of the researcher was statistically significant
The topic of seniority also emerged clearly from the interviews conducted, although under a different and less-flattering perspective. Most interviewees considered that seniority, in relation to researchers’ track-record of acquired work and number of publications, enables researchers to wield power over younger researchers which can result in both questionable and unfair practices. An unfair practice that was frequently discussed in interviews, as illustrated by the quote below, relates to unfair publication agreements between junior and senior-level researchers which devoid science of any potential societal value and impact.
There’s also practice those who are senior, it doesn’t matter how much they contribute, they want to be the first author. (…) Because, first of all to tell that because I am the Principal investigator, I have to be the first author of every single paper, it doesn’t matter, whoever, right? Because I brought the grant. I’ve experienced that. So the thing that I brought the grant, so I should be the first author. (…), (GS4)
Another potential reason for age discrepancies in URPs was the more recent nature of decolonising debates, resulting in junior researchers potentially being more sensitised and committed to FRP.
Related to the issue of seniority, many participants reported that concerns of career progression may incentivise Global Health researchers to engage in unfair and questionable behaviours. Interestingly, this finding was discussed mostly in relation to Global North researchers, and practices concerning fair involvement of Global South partners in the research preparation as well as dissemination and communication stage.
I really think that it’s much easier for (a)Western person to come to our settings and get something published. Maybe I can bring another example. You know, I was talking with someone from the North, who just came to Uganda for one-year research fellowship and then just chatting, I asked the motivation and she was like, well, but you can come here in one year, I can pull out easy, easy 2-3 papers, you know, and then I can start my career from there. So you see. Hey, there is definitely, there is less competition, it’s easy to maybe write up maybe in some institutions that you know it’s easier to get data because (…) they have no policy on data sharing and stuff like that. (…) They asked for the data, you gave it to them. (GS1).
While this quote describes Global North researchers taking advantage of their access to data for individual benefit, some also stressed what interviewee GX1 described as ‘laziness to go the extra mile’; that is, taking the time to cocreate and cede decision-making power on the use and sharing of data.
Several interviewees also pointed to language skills, an individual determinant that can be connected to structural factors around access to quality education as well as institutional factors such as the lack of linguistic diversity in the sector’s working language and within academic journals. Language skills reportedly affect both the role of Global South researchers acting (predominantly) as data collectors given their knowledge of local languages as well as being less involved in the write-up of study results, arguably because Global North partners possess stronger English language skills. Some participants also touched on another individual factor which affects (not) publishing results, being the researchers’ pride or fear of missing potential future funding opportunities associated with mentioning study flaws, limitations or negative findings.
Discussion
Overall, researchers reported mostly adhering to research integrity and research fairness principles with little geographical variation. Some behaviours are more frequently reported (transparent reporting of studies, seeking local ethical approval) than others (engagement with affected populations, engagement with local decision-makers, adherence to Open Science), with little variation between responses from Global North and Global South. However, there are some small yet significant differences in specific practices (individual questions of the survey) with Global South researchers generally more likely to report desirable practices, such as giving sufficient attention to skills and expertise, sufficiently mentoring their junior coworkers, consulting representatives of affected populations, consulting end-users of research, having clear decision-making processes agreed on, having clear and fair data ownership agreements and experiencing strategies in place to encourage secondary analyses.
Several structural factors were associated with these patterns, such as an inflexible donor landscape leading to time and resource pressure and competition. This was found to exacerbate tendencies to allocate unequal roles and responsibilities between Global North and Global South researchers that are rooted in pervasive neocolonial mentalities. However, institutional factors were also seen as important determinants, such as universities’ and research institutions’ investments in relationship building, efforts to develop and ensure adherence to guidelines and commitment to mentoring students or junior staff. Our regression analyses did not provide convincing evidence that individual determinants affect research practices, but interviews revealed that senior researchers at times enact power over younger researchers resulting in both questionable and unfair practices. Similarly, neocolonial superiority complexes were also found to explain unfair practices.
Overall we found that there are more synergies than trade-offs between research integrity and fairness as they share similar structural determinants (competitive landscape leading to time and resource pressure and competition), institutional determinants (investments in relationship building, efforts to develop and ensure adherence to guidelines, commitment to mentoring supervising of students or junior staff) and individual determinants (power differentials and competition between senior and junior researchers). This is clearly exemplified by the ‘helicopter research’ projects led by insufficiently supervised far-away supervisors (a classic threat to research integrity) but seen as key for career progression because they enable ‘quick and low-cost’ publication returns (a clear example of extractive research). Another example is data fabrication—the research integrity violation ‘par excellence’—which can be the result of financial constraints in unfair partnerships (either at the individual or project level) that put pressure on researchers in LMICs to fabricate patients and pocket financial reimbursements. This is in line with other studies that have also shown that integrity and fairness are not mutually exclusive goals. Indeed, the disproportionate and unfair distribution of decision-making power within research partnerships29 can weaken the design of research processes and tools, even in the task of properly soliciting informed consent from research participants.33 Given that both integrity and fairness share not only determinants leading to these practices but also a goal of increasing both research quality and the societal benefits of research, there is ample scope to make such synergies explicit and to align both agendas in international research collaborations, as has been advocated by the recently published Cape Town Statement on research integrity.2
The only trade-off that emerged between research integrity and research fairness agendas concerns Open Science and data-sharing. In general, practices related to Open Science (publishing under Open Access conditions as well as making data and programming code openly available) were found to be least frequently reported. This is not surprising for at least two reasons. First, much global health research relies on a mixture of quantitative and qualitative research methods. Yet it can be difficult to anonymise qualitative data when participants provide detailed information about their personal experiences and in such cases removing personal identifiers may not be enough to ensure anonymity. Second, there is a literature showing that Open Science practices are problematic in global health7 34 as they can exacerbate existing inequities between regions. Indeed, as argued in a recent review, open research processes can only lead to wide reuse or participation if there is strong pre-existing capacity to do so (in terms of knowledge, skills, financial resources, technological readiness and motivation). If that is not the case, Open Science risks mostly helping researchers in higher income countries get published, who did not share the ‘legwork’34 in collecting data but have access to higher analytical capacities (eg, students able/willing to do free internships, better computing power) and financial resources (institutional funds to pay article processing charges for spin-off research ideas). Our results are not clear-cut but in line with these concerns. Indeed, in addition to finding rather low adherence to Open Science practices, we also found that strategies were only occasionally put in place to encourage secondary analyses by local researchers according to Global North researchers (though interestingly Global South researchers reported that this happened frequently).
Although there are few studies looking at determinants of research integrity or fairness in global health, those that exist primarily focus on the former. In line with previous studies,15 we found some evidence that junior researchers are less likely to adhere to responsible research practice compared with senior researchers. This is expected as junior researchers are meant to grow into research and collaboration. However, this was not corroborated by the qualitative research which showed that senior levels researchers were more likely to have URPs, especially relating to unfair publication agreements. A recent qualitative study of global health research partnerships also outlined many factors affecting research integrity identified in our study, including the competitive culture of academia, the scarcity of long-term research grant funding, institutional cultures and power dynamics between junior and senior researchers, and lack of research integrity training.35 While that study primarily focused on practices linked to research integrity, they also describe unfair practices related to authorship, and the conflicts that can occur between Global North and Global South partners over fair attribution. Other studies of fairness in global health research have not sought to identify its determinants as we have but explored dynamics of international research partnerships that were reported as contributing factors in this study. The extractive nature of research conducted in the Global South by researchers from the Global North has been clearly argued in a study that linked between (research) data to gold and researchers and gold diggers.36 For example, even where global health research partnerships are ‘supposed’ to lead to ‘North to South transfers of financial and material resources’ macrolevel differences in power and resources end up being reproduced by the institutions, research teams and individuals that make up the partnerships.37 Even setting up such partnerships equitably can be complicated when northern funders set limits on indirect costs or overheads for the southern partner.38 Thus, while equity remains the aim for many global health research partnerships, a de facto reality is established with entrenched institutional arrangements, which extends to the division of roles across partners. Reports of Global South researchers ‘being relegated to tasks well below their capacity’ with ‘no opportunity to participate in priority-setting or in leadership roles’ are common.39 The main strength of our study is the scientific rigour of the study design, but limitations include our low response rate and associated biases. Indeed, we applied a robust epidemiological design for the frequency study based on two-stage random sampling of researchers clustered within institutes from a broad range of research networks worldwide. Latin American as well as Francophone and Lusophone African institutes are absent from our sample (apart from Cote D’Ivoire) due to their limited representation in the networks that contributed to the sampling frame. To the best of our knowledge, this is the first epidemiologically rigorous study on research fairness (although there are more examples in the field of research integrity). Moreover, we were able to combine the breadth of evidence from a global survey with the depth of knowledge obtained from interviews. Despite the small sample size, we were able to reach saturation and triangulate information on several important survey themes. However, our study suffered from a low response rate, with only 8.4% of researchers contacted via email filling in the survey. This is a well-known issue for research integrity surveys (the Dutch National Research Integrity Survey had a response rate of 21.2%15 while the survey of European and American researchers had a response rate of 7.2%40) and can be ascribed to time constraints, survey fatigue, lack of perceived relevance, trust and privacy concerns. Furthermore, we cannot exclude the possibility of positively biased responses since our study measured self-reported adherence to research practices that are well known to be either desirable or not desirable. On a more subtle level, there is also the possibility of an ‘intention-action gap’: no one is against fairness and integrity, but it often takes courage and deliberate actions to consistently act on one’s principles. Lastly, especially, considering that the response rate was different between Global North (6.2%) and Global South (9.5%), it is possible that each stratum represents a different subset of researchers, meaning the differences in scores we found between the two groups may reflect differences between these subgroups rather than ‘population-level’ differences (differential bias).
There are also some limitations pertaining to the survey tool. First, we did not determine the prevalence of research fairness and integrity, as initially intended per protocol, due to the measurement scales used. Indeed, survey questions measured the frequency of researchers’ involvement in specific practices (never, very rarely, rarely, occasionally, frequently, very frequently and always), rather than binary responses (yes, no). With hindsight, we did not feel comfortable collapsing the frequency variables into two categories as this would mean substantial data loss. As a second limitation related to our tool, some variables are more likely to generate valid responses as they incorporate specific and verifiable details about desired behaviours (eg, whether end users were consulted for dissemination products or whether researchers made material accessible on Open Science platforms). Conversely, other questions were based on subjective judgements (eg, allocation of authorship as ‘fair’ or mentorship as ‘insufficient’).
Our study has several implications for practice. Taking individual accountability as a starting point, our findings underline the importance of regular training, coaching and mentoring for global health researchers, for both junior and senior staff, ensuring exposure to up-to-date practices related to research integrity that also address issues of biases and privileges. For strengthened institutional commitment, academic institutions could prioritise investments in training as well as guideline development and adherence to ethical and FRPs. Next to the individual and institutional determinants, funding policies and inequities in the funding landscape need to be addressed at scale, as flexible and equitable practices can hopefully drive more equal power dynamics between Global North and Global South researchers and instil good practices in global health research. Overall, more scientific research on this topic will be key to taking an evidence-informed approach to tackling research fairness and integrity, for instance, providing qualitative insights to document and learn from good practices for counteracting the individual, institutional and structural determinants affecting research fairness and integrity.
Conclusion
To the best of our knowledge, this is the first study providing empirical evidence using rigorous research methods to study research fairness and integrity in global health. Our study suggests that global health researchers mostly adhere to research integrity and research fairness principles (with little geographical variation) but structural, institutional and individual factors are a barrier to following ‘ideal’ practices. Our study shows there is ample scope to align research integrity and research fairness agendas in global health, as only science that is conducted with fairness can be considered responsible and conducted with integrity. This is underscored by the fact that there are more synergies than trade-offs between research integrity and research fairness as they share similar determinants. These include structural factors, such as inflexible donor landscapes and neocolonial mentalities, and unequal roles and responsibilities between Global North and Global South researchers. In practice, our study emphasises the need for institutional and structural initiatives to promote research integrity that also address issues of biases and privileges, foster equal partnerships and address funding inequities, to promote good practices in global health research.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request and will be delinked from the study participants.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by KIT Research Ethics Committee approval, with application number (S-181). KEM Hospital Research Centre Ethics Committee and the ref no is KEMHRC/RVMlECI 24. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are very grateful to Lonneke van der Waa and Lindy van Vliet for making this study possible. Many thanks to Carel IJsselmuiden and Sanjay Juvekar for insightful inputs during the conception stage of this study.
[ad_2]
Source link
Punjab inmates granted relief

[ad_1]
RAWALPINDI:
President Asif Ali Zardari and Punjab Chief Minister Maryam Nawaz Sharif on Sunday have granted relief to the prisoners in the province’s jails keeping in view the holy month of Ramazan, releasing 28 of them while reducing the sentences of others by 90 days.
The officials announced that 2,367 inmates across the province benefited from the reduction in their sentences.
However, they added that the prisoners involved in cases of drugs, adultery, robbery, kidnapping, rebellion and espionage would not receive this concession.
Similarly, this reduction in punishment has not been applied to the prisoners involved in financial embezzlement and damage to the national exchequer.
It applies to the male inmates who are 65 years of age or older and served one-third of their sentence as well as the female prisoners who are 60 years of age or older and served one-third of their jail time.
The concession also applies to the female prisoners who are accompanied by children as well as juveniles, who are below the age of 18 and served one-third of their sentence.
Read also: President approves remission for prisoners
According to the officials, nine inmates were released from six prisons across the Rawalpindi region – six from Adiala Jail, two from Jhelum and one from Gujrat.
Besides, 642 prisoners in all the six jails of Rawalpindi region – Adiala, Gujrat, Attock, Jhelum, Mandi Bahauddin, and Chakwal – received the benefit of the special amnesty and their sentences were reduced.
Punjab IG Prisons Mian Farooq Nazir said the prisoners confined in the jails of the province and their families expressed their happiness on the announcement of the reduction of the sentences.
He added that they expressed their gratitude to the president, premier and Punjab chief minister for this move.
Earlier this month, the federal government, with the approval of PM Shehbaz, announced a significant sentence reduction for prisoners across the country.
Read: CM Maryam announces release of 155 prisoners
According to a notification, the government has given a two-year remission to convicted prisoners in their jail terms.
It is customary to grant relief to prisoners during the holy month of Ramazan.
Last year, the then president Dr Arif Alvi announced a 90-day reduction in the sentences of prisoners on the occasion of Eidul Fitr when the holy month concluded.
The number of inmates who benefited from the president’s special amnesty stood at 2,610. A total of 39 prisoners were released from Rawalpindi’s Adiala Jail while 415 had their sentences reduced.
According to a statement from the President’s House, Alvi approved the reduction on basis of Article 45 of the Constitution.
Article 45 mandates that the president holds the “power to grant pardon, reprieve and respite, and to remit, suspend or commute any sentence passed by any court, tribunal or other authority”.
[ad_2]
Source link
It Is Possible to ‘Poison’ the Data to Compromise AI Chatbots With Little Effort

[ad_1]
According to researchers, individuals could potentially disrupt the accuracy of AI chatbots by intentionally contaminating the datasets upon which these systems rely, all for a minimal cost.

Coding a chatbot – illustrative photo. Image credit: James Harrison via Unsplash, free license
As it stands, AI chatbots already exhibit biases and deficiencies attributable to the flawed data on which they are trained. The researchers’ investigation described on Business Insider revealed that malevolent actors could deliberately introduce “poisoned” data into these datasets, with some methods requiring little technical expertise and being relatively inexpensive.
A recent study conducted by AI researchers unveiled that, with as little as $60, individuals could manipulate the datasets essential for training generative AI tools akin to ChatGPT, which are crucial for providing precise responses.
These AI systems, whether chatbots or image generators, leverage vast amounts of data extracted from the expansive digital realm of the internet to generate sophisticated responses and images.
Florian Tramèr, an associate professor of computer science at ETH Zurich, highlighted the effectiveness of this approach in empowering chatbots. However, he also underscored the inherent risk associated with training AI tools on potentially inaccurate data.
This reliance on potentially flawed data sources contributes to the prevalence of biases and inaccuracies in AI chatbots. Given the abundance of misinformation on the internet, these systems are susceptible to incorporating erroneous information into their responses, further undermining their reliability and trustworthiness.
Through their investigation, researchers discovered that even a “low-resourced attacker,” armed with modest financial resources and sufficient technical expertise, could manipulate a relatively small portion of data to substantially influence the behavior of a large language model, causing it to produce inaccurate responses.
Examining two distinct attack methods, Tramèr and his colleagues explored the potential of poisoning data through the acquisition of expired domains and manipulation of Wikipedia content.
For instance, one avenue for hackers to poison the data involves purchasing expired domains, which can be obtained for as little as $10 annually for each URL, and then disseminating any desired information on these websites.
According to Tramèr’s paper, an attacker could effectively control and contaminate at least 0.01% of a dataset by investing as little as $60 in purchasing domains. This equates to potentially influencing tens of thousands of images within the dataset.
The team also explored an alternative attack strategy, focusing on the manipulation of data within Wikipedia. Given that Wikipedia serves as a “crucial component of the training datasets” for language models, Tramèr emphasized its significance in this context.
According to the author, Wikipedia prohibits direct scraping of its content, instead offering periodic “snapshots” of its pages for download. These snapshots are captured at regular intervals, as publicly advertised on Wikipedia’s website, ensuring predictability in their availability.
Tramèr’s team outlined a relatively straightforward attack approach involving strategically timed edits to Wikipedia pages. Exploiting the predictable nature of Wikipedia’s snapshot intervals, a malicious actor could execute edits just before moderators have an opportunity to revert the changes and before the platform generates new snapshots.
This method allows for the surreptitious insertion of manipulated information into Wikipedia pages, potentially influencing the content used to train language models without raising immediate suspicion.
Tramèr suggests hat at least 5% of edits orchestrated by an attacker could successfully infiltrate the system. However, the success rate of such attacks would likely exceed 5%, he said.
Following their analysis, Tramèr’s team shared their findings with Wikipedia and proposed measures to enhance security, such as introducing randomness into the timing of webpage snapshots, mitigating the predictability exploited by potential attackers.
Written by Alius Noreika
[ad_2]
Source link
African polyvalent antivenom can maintain pharmacological stability and ability to neutralise murine venom lethality for decades post-expiry: evidence for increasing antivenom shelf life to aid in alleviating chronic shortages
[ad_1]
Introduction
Snakebite envenoming, a WHO-recognised neglected tropical disease,1 is thought to cause approximately 81 000–138 000 deaths each year while permanently disabling a further 400 000 people.2 The victims of snakebite envenoming are overwhelmingly the poorest populations living in some of the most resource poor regions of the world.3 As it stands, the only established therapy for snakebite envenoming is antivenom, a polyclonal mixture of antitoxin antibodies refined from the sera of venom of hyperimmunised horses or sheep.
Antivenoms, like all therapeutics, have a defined shelf life. The WHO definition of shelf life is ‘the period of time, from the date of manufacture, that a product is expected to remain within its approved product specification while handled and stored under defined conditions’.4 For antivenoms, which are biologics, this period typically ranges from 2 to 5 years depending on the specific product, and is validated by testing the retention of key pharmacological, physicochemical, immunochemical and microbiological properties during the specified storage period. Once an antivenom has expired, it is outside the window of stability testing undertaken by the manufacturer, and thus the safety and effectiveness of the product become uncertain.
There have been critical shortages in antivenom supply for several decades.5–7 The shortages are a global phenomenon, but it is the regions in greatest need and most under-resourced that suffer the most acute shortages.6 8 Sub-Saharan Africa is the most notable example of this, with several antivenom market failures and frequent product stockouts, leading to extremely limited to no antivenom provision in large swathes of the continent.8–10 However, despite the shortfall in overall doses available, substantial quantities (up to 50% in one reported locale) of antivenom actually exceed their expiry dates and are subsequently discarded.11–13 The cause of this waste of critically precious antivenom is mainly due to difficulties in the national and regional antivenom inventory management, due to a lack of research and information around national requirements, weak infrastructure and financial inaccessibility, issues which are being actively addressed by various stakeholders.14–16
Considering the global crisis in antivenom supply, the loss of antivenom due to expiry has driven investigation into whether expired antivenoms retain clinical efficacy, with the rationale that they could be used in emergency situations when in-date antivenom is unavailable. It is widely recognised in academic settings that antivenoms can retain their efficacy for many years after their expiration, with several recent studies demonstrating retained antivenom preclinical efficacy, similar to that of non-expired antivenom, up to two decades post-expiry.17–20 Furthermore, there is clinical precedent for the use of expired antivenom in certain situations. For example, the US Food and Drug Administration (FDA) approved the use of expired North American coral snake antivenom after it was discontinued by its manufacturer Wyeth in 2006.21 In emergency cases, the use of ‘recently’ expired antivenom is recommended by the WHO if no other option is available.22 This advice seems to be reflected in practice, with reported cases of expired antivenoms being used in several countries, perhaps routinely, when in-date antivenoms were not available, with reported positive outcomes.23 24 The most extensive report detailing the use of expired antivenom was a clinical study of 31 patients suffering from systemic effects of envenoming in the Lao People’s Democratic Republic.25 The patients in this study received antivenom which was beyond expiry by 1–6 years, as a result of the unavailability of in-date antivenom within the country at the time.25
In the studies to date, there has been limited evaluation of the neutralising capacity of expired antivenom products for sub-Saharan Africa, arguably the region with the greatest antivenom supply crisis, with just a single study identified.19 South African Institute for Medical Research (SAIMR) polyvalent, manufactured by South African Vaccine Producers (SAVP), is currently the only polyvalent antivenom produced within sub-Saharan Africa15 and throughout its 50-year history, it has enjoyed a good reputation of clinical efficacy, despite limited published evidence to support this.26 Here, we present a preclinical analysis of the venom neutralising characteristics of expired SAIMR polyvalent antivenom, using eight expired batches going back to 1991 and using several of the most medically important venoms from the region. We also report on immunochemical analyses of product stability of these batches, using industry standard quality control assessments. Our findings demonstrate that SAIMR polyvalent can retain preclinical efficacy and maintain acceptable product stability up to 25 years after its stated expiry date.
Methods
Additional detailed descriptions of all of the materials and methods used in this study are provided in the online supplemental methods.
Antivenoms
For this study, we used the SAVP equine F(ab’)2 polyvalent antivenom, ‘SAIMR polyvalent antivenom’. SAIMR polyvalent is manufactured from horses that have been hyperimmunised with the venoms of Bitis arietans, B. gabonica, Hemachatus haemachatus, Dendroaspis angusticeps, D. jamesoni, D. polylepis, Naja nivea, N. melanaluca and N. mossambica. According to the product insert, SAIMR polyvalent antivenom is indicated as ‘effective against the venoms of the rinkhals, mambas, and all the cobras and vipers likely to cause life-threatening envenoming in Africa’. All SAIMR polyvalent antivenom used in this study was donated by the UK Health Security Agency (or its predecessors) shortly after its expiry date. Antivenoms were stored long term, unopened in their original sealed glass ampules, at 4°C. Eight batches of antivenom were used with the following expiry dates (month/year) and lot numbers: 08/1991 (lot A706 S1), 08/1994 (lot D04446), 07/1997 (lot G03146), 11/2000 (lot J06646), 09/2001 (lot K04846), 09/2012 (lot X02646), 07/2015 (lot BB01446), 11/2017 (lot BF00546). Transport of two vials of each batch of antivenom from Liverpool School of Tropical Medicine (LSTM) to Instituto Clodomiro Picado (ICP) was through a specialist courier service (Biocair) with uninterrupted refrigerated conditions (2–8°C) throughout. All vials were used immediately after opening. Prior to being opened, each ampoule was inspected for visual differences in its content. This included noting the colour and if there were any visible particulates of precipitates in the liquid. Due to limited quantity of antivenom of each batch available for analysis, all results below are representative of technical replicates (from single vials) only.
Venoms
LSTM venoms: venoms used in ELISAs and in vitro snake venom metalloproteinase (SVMP) and phospholipase A2 (PLA2) assays were obtained from wild-caught specimens maintained in, or historical venom samples stored in, the Herpetarium of the LSTM. Following collection, venoms were immediately frozen and lyophilised to be stored as a powder at 4°C. Venoms were reconstituted in phosphate-buffered saline (25 mM sodium phosphate, 0.15 M sodium chloride (NaCl), pH 7.4) and stored at a concentration of 1 mg/mL at −20°C, unless stated otherwise. Venoms were only freeze-thawed once prior to use. Venoms used were pooled from multiple extractions of the following species: B. arietans (origin: Kenya), D. polylepis (Tanzania), N. haje (Uganda), N. nigricollis (Tanzania) and H. haemachatus (South Africa).
ICP venoms: venoms of adult specimens of B. arietans (unspecified origin, batch #322.061), D. polylepis (unspecified origin, batch #416.031) and N. nigricollis (unspecified origin, batch #616.031) were purchased from Latoxan (Portes-dès Valence, France). After collection, venoms were stabilised by lyophilisation and stored at −40°C. Solutions of venoms were prepared in 0.9% NaCl injection USP, immediately before use.
Nephelometric turbidity
Turbidity of antivenoms was measured at ICP in 2023. Nephelometric turbidity of antivenoms, expressed as nephelometric turbidity units (NTUs), was assessed as per US Pharmacopeia specifications.27 Briefly, samples of antivenoms were placed in reading cells and analysed in a LaMotte 2020 Turbidimeter (Chestertown, Maryland, USA) through comparing the intensity of light scattered by the sample with the intensity of the light scattered by a reference solution. Assays were performed in triplicate and results expressed as mean±SD.
SVMP assay
The SVMP assay was performed at LSTM in 2022 as previously described.28 29 Briefly, 1 µg of venom in a 1 µL volume was added to each well, followed by 10 µL of antivenom diluted in assay buffer (150 mM NaCl, 50 mM Tris pH 7.5). Antivenom dilutions of 1 in 4, 1 in 8 and 1 in 16 were used. The negative control was assay buffer alone. Each condition was performed in quadruplicate on a 384-well plate (Greiner Bio-One). The plates were briefly spun at 2500 rpm and then incubated for 25 min at 37°C, and for a further 5 min at room temperature. 90 μL of a quenched fluorogenic substrate (ES010, R&D Biosystems, supplied as a 6.2 mM stock) was then added to each well using a Multidrop Combi (Thermo-Scientific), and reactions monitored using a CLARIOstar Plus plate reader (BMG Labtech) at 420 nm for 75 min (10 flashes/well, 100 cycles) at an excitation wavelength of 320 nm and emission wavelength of 405 nm. The measurements at 52 min were chosen as the endpoint as all fluorescence curves had plateaued by this time point. Raw data were recorded in MARS data analysis software (BMG Labtech) prior to export and analysis in GraphPad Prism V.9. Results were then expressed as a percentage of the venom-only SVMP activity.
PLA2 assay
The PLA2 assay was performed at LSTM in 2022. The antivenoms were tested using the commercial Abcam sPLA2 assay (Abcam) optimised for high-throughput screening.30 The final reaction consisted of 9 µL each of the antivenoms (n=8) against 1 µL of each snake venom plated out into a 384-well plate (Grenier Bio). For H. haemachatus and N. nigricollis, stock solutions of 10 mg/mL were diluted 1 in 2000, resulting in 5 ng of venom per reaction. Following incubation of the venom and antivenoms for 30 min at 37°C protected from light, the plate was acclimatised for 5 min to room temperature. 5 µL of a stock of 4 mM 5,5′-Dithiobis(2-nitrobenzoic acid) (DNTB) in distilled water was added to each well of the venom+antivenom plate. The substrate 1 mM stock was prepared by resuspending in 1X assay buffer (diluted from the 10X stock in MilliQ water: 25 mM Tris-hydrogen chloride, pH 7.5, 10 mM calcium chloride, 100 mM potassium chloride, 0.3 mM Triton X-100). The addition of 30 µL of the substrate solution per well resulted in a final reaction concentration of 0.89 mM. The addition of venom, DTNB and substrate was done using a VIAFLO384 liquid handler (Integra). Following the addition of the substrate, the plates were immediately read kinetically on a CLARIOstar plate reader at 405 nm for 15 min (settings for a full 384-well plate were 11 flashes, 161 s cycle time). Raw data were recorded in MARS data analysis software prior to export and analysis in GraphPad Prism V.9. Results were then expressed as a percentage of the venom-only PLA2 activity.
In vivo neutralisation of venom-induced lethality
Sample size determination
We used the WHO-recommended essential in vivo preclinical assay to evaluate the ability of expired antivenoms to neutralise venom-induced lethality.31 This assay stipulates minimum numbers of animals required per assay to gain statistical significance and normal data distribution via Probit analysis of the median effective dose (ED50).32 This requires data from five experimental groups (consisting of five experimental units, that is, five mice), which receive a fixed dose of venom with a variable dose of antivenom. The groups are required to have one group with all survivors, one with all deaths and three groups with some survivors and some deaths. Therefore, five experimental groups are required for each ED50 assay. To determine the in vivo efficacy of each of the eight antivenoms versus three medically important venoms requires 24 assays (600 mice).
Animal maintenance
CD1 mice weighing 20–22 g, of both sexes, were obtained from the Bioterium of ICP. Mice were housed by sex in randomly allocated groups of five in Techniplast Eurostandard Type II 1264C cages (L25.0×W40.0×H14.0 cm) and maintained at 18–24°C, 60–65% relative humidity and 12:12 light-dark cycle, with food and water available ad libitum.
Neutralisation of lethality assessment
All experiments used mixed genders, and experimenters were unblinded to the test articles. Mice were pretreated with the analgesic tramadol, administered subcutaneously, at a dose of 50 mg/kg,33 15 min prior to administration of venom challenge. Mice were then injected intravenously with mixtures containing a challenge dose of venom dissolved in sterile 0.9% NaCl USP injection solution and variable dilutions of antivenom, which were premixed and incubated at 37°C for 30 min (volume of injection was 0.2 mL).34 Challenge doses were three times the previously determined median lethal dose (LD50) for the venoms of N. nigricollis (3× LD50=55.2 µg/mouse)35 and D. polylepis (3× LD50=1.14 µg/mouse)36 and five times for the venom of B. arietans (5× LD50=110 µg/mouse).37 The rationale for using 3× LD50 challenge doses for N. nigricollis and D. polylepis, rather than the conventional 5× LD50, was a refinement due to experience with these particular venoms demonstrating the use of 5× LD50 resulted in poor resolution of dose groups outcomes. The number of resulting deaths was recorded at 6 hours.38 The ED50 and the corresponding 95% CIs were calculated by Probit analysis.32 In line with recent WHO recommendations to report in vivo antivenom efficacy outcomes using the potency metric39 (the amount of venom completely neutralised per millilitre of antivenom (mg/mL), resulting in 100% survival of test animals40), calculated ED50 values were used to determine potency using the following equation: p=n–1 LD50/ED50, where n=the number of LD50 in the challenge dose.
Results
Total protein concentration
Total protein concentration of the eight antivenoms was determined by Biuret assay and ultraviolet/visible (UV/VIS) spectrometry. Concentrations measured by the two methods were consistent overall, although the OD280 nm measurements typically reported lower concentrations than Biuret, with no trend in protein concentration over time apparent (figure 1A). Total protein concentration ranged from a low of 121 mg/mL (1994) to 157 mg/mL (2000) by Biuret (mean=142 mg/mL, SD=11 mg/mL) or 121 mg/mL (1994) to 146 mg/mL (2000) by UV/VIS spectrometry (mean=129 mg/mL, SD=9 mg/mL).
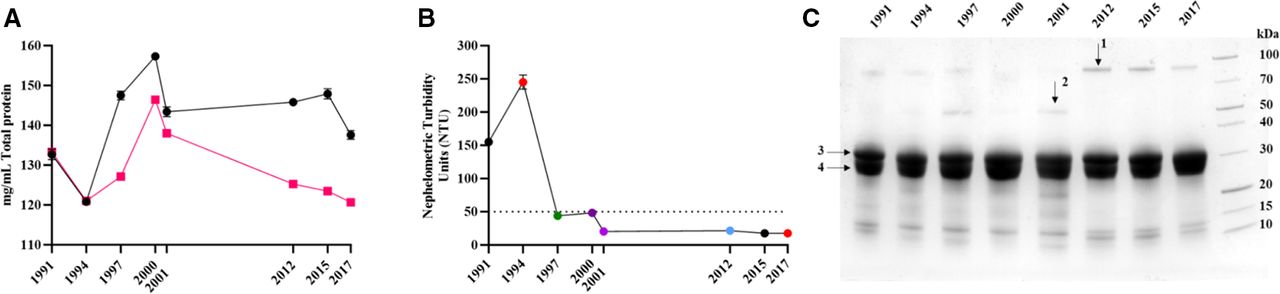
Physiochemical analysis of expired SAIMR polyvalent antivenoms. Antivenom expiry year is represented on each x axis. (A) Mean (n=3 technical replicates) total protein concentration (mg/mL) of each batch determined by Biuret (black points) or Nanodrop (red points). Error bars represent the ±SD. (B) Nephelometric turbidity assessment of each batch of antivenom expressed as mean (n=3) nephelometric turbidity units (NTUs). Error bars represent the ±SD. The dotted line represents 50 NTUs, the maximum permitted NTU for antivenom manufactured at Instituto Clodomiro Picado. (C) Reducing SDS-PAGE profiles of expired SAIMR polyvalent antivenom batches (denoted by year of expiry along top) centrifuged and the resulting supernatants diluted 1/75 prior to loading. Arrows represent bands analysed by mass spectrometry. 1=alpha-1-antitrypsin, 2=alpha-2-macroglobulin, 3 and 4=immunoglobulin fragments representative of antibody heavy and light chains, respectively. SAIMR, South African Institute for Medical Research.
Turbidity
Visual inspection of the eight unopened antivenom vials revealed the oldest vial (1991) appeared cloudy with fine particulate matter, while the 1994 expiry antivenom appeared to have larger particulate matter but were transparent and pale yellow in colour. The remaining six antivenoms were transparent and pale yellow in colour. Nephelometric turbidity analysis reflected this, with elevated values for the oldest vials from 1991 and 1994, but acceptable levels of turbidity (<50 NTUs) for the remaining eight vials despite the time lapsed after their expiry (figure 1B).
Protein profiles
SDS-PAGE profiles of all antivenoms and GFC of four antivenoms demonstrated that >90% of the antivenom protein content corresponds to F(ab’)2 immunoglobulin fragments (ie, the active ingredients) (figure 1C). Overall, results did not demonstrate any substantive evidence of immunochemical degradation over time. Additional bands and peaks not corresponding to F(ab’)2 fragments were visible in both SDS-PAGE and GFC. Mass spectrometry identification of these additional bands reveals they are the common serum proteins alpha-1-antitrypsin and albumin. GFC also revealed an additional peak at 214 nm but not at 280 nm, indicating that it is not proteinaceous in nature (online supplemental figure 1).
ELISA and immunoblotting
Next, we examined the ability of antivenoms to recognise, via ELISA, five key African venoms; B. arietans, H. haemachatus, D. polylepis, N. haje and N. nigricollis. All expired antivenoms were able to recognise the five venoms (figure 2 and online supplemental figure 2), with examination of the absorbance at OD405 nm at a dilution of 1 in 1250, representing a dilution mid-titration curve, proving to be consistent over time (figure 2A). Immunoblotting against the same venoms suggested that there was an overall decrease in recognition of venoms by all antivenoms which expired from 1991 to 2001, as compared with antivenoms which expired in 2012, 2015 and 2017 (online supplemental figure 3).
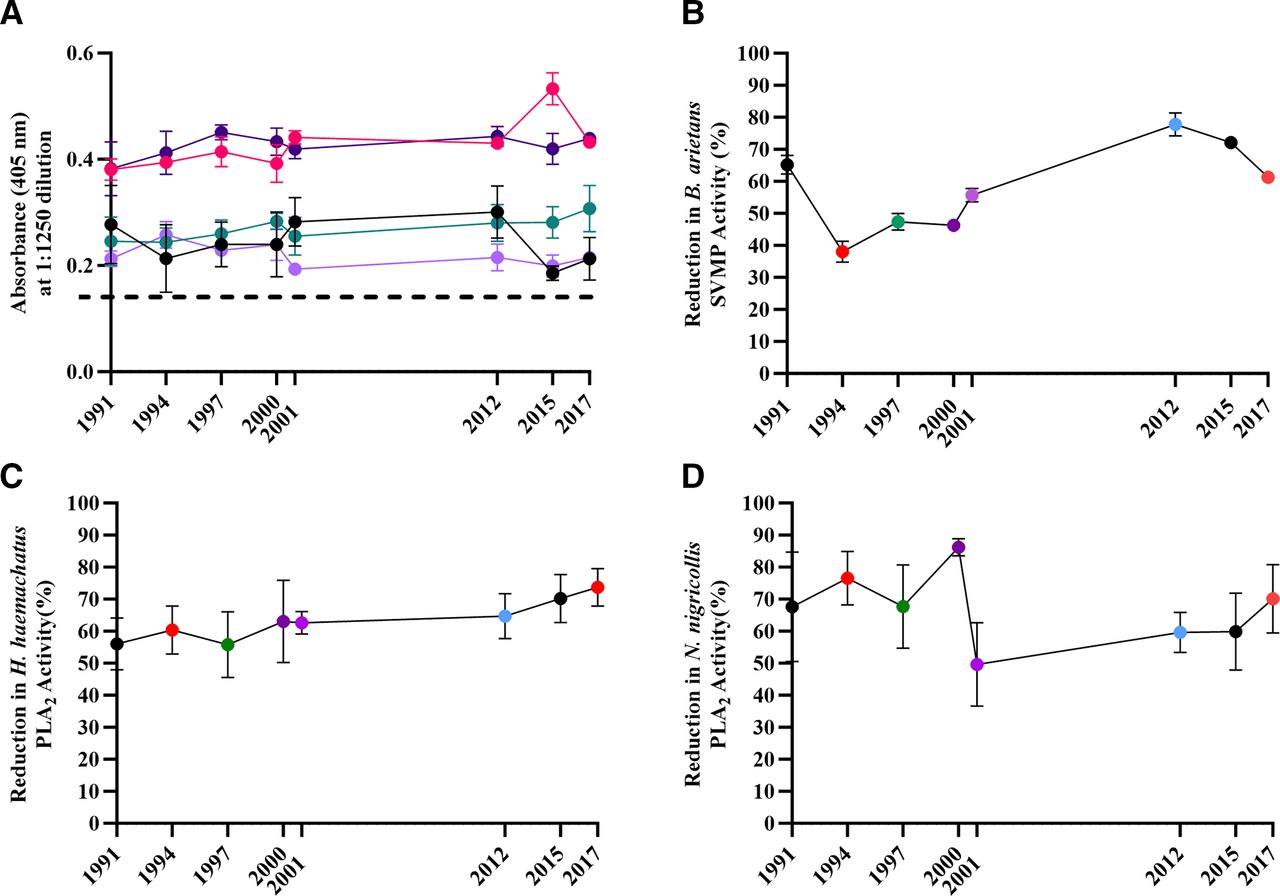
In vitro preclinical analysis of expired SAIMR polyvalent batches. Antivenom expiry year is represented on each x axis. (A) Mean (n=3 technical replicates) antibody titre at a neat antivenom dilution of 1:1250, expressed as absorbance at 405 nm. Error bars=±SD. Light purple =Bitis arietans venom, dark purple =Dendroaspis polylepis, red =Hemachatus haemachatus, green =Naja haje, black =N. nigricollis, dashed line=blank (PBS). (B) Ability of each antivenom to inhibit in vitro SVMP activity of B. arietans venom. Results represent mean (n=3 technical replicates) % inhibition compared with activity of venom-only controls. Error bars=±SD. (C,D) Ability of each antivenom to inhibit in vitro PLA2 activity of H. haemachatus (C) and N. nigricollis (D). Points represent mean (n=8 technical replicates) % inhibition compared with the activity of venom-only controls. Error bars=±SD. PBS, phosphate-buffered saline; PLA2, phospholipase A2; SAIMR, South African Institute for Medical Research; SVMP, snake venom metalloproteinase.
Antivenom in vitro neutralising capacity
We subsequently investigated the ability of the expired antivenoms to neutralise toxin-specific activity in biochemical functional assays, specifically PLA2 activity (in H. haemachatus and N. nigricollis venoms) and SVMP activity (in B. arietans venom).
The SVMP activity of B. arietans venom was inhibited by all antivenoms to varying extent, with the 2012 expiry antivenom having the most potent SVMP-inhibiting activity (77.8%), while the 1994 batch possessed the lowest level of SVMP inhibition (38.0%) (figure 2B). There is a gradual reduction in B. arietans SVMP-inhibiting capability in ageing antivenoms from 2017 to 1994. However, the oldest antivenom (1991 expiry) has a greater inhibiting capability than the majority of antivenoms, with the exception of the 2012 and 2015 expiry.
The functional PLA2 activity of both H. haemachatus and N. nigricollis was inhibited by all antivenoms to varying extent (55.8–73.7% for H. haemachatus and 49.7–86.2% for N. nigricollis) (figure 2C,D). However, the capability of individual expired antivenoms in inhibiting either H. haemachatus or N. nigricollis PLA2 activity was not consistent across the two venoms. The PLA2-inhibiting capacity of the antivenoms versus H. haemachatus venom steadily reduced as the antivenoms aged (figure 2C), while antivenoms which expired in or before 2000 appeared substantially more capable of inhibiting N. nigricollis PLA2 activity than the more recently expired antivenoms (figure 2D).
Antivenom in vivo neutralising capacity
With the demonstration that expired antivenoms retained in vitro venom toxin neutralising capability, despite substantial time passing since expiry, we proceeded to determine the murine in vivo ED50 and subsequently the potency, of each expired antivenom. Using the WHO-recommended essential in vivo preclinical assay to measure antivenom neutralisation of venom-induced lethality,31 we assayed three medically important venoms (B. arietans, D. polylepis and N. nigricollis) whose envenoming is indicated for treatment by SAIMR polyvalent. Results demonstrate all antivenoms retained their ability to neutralise the systemic lethal effects of each venom (figure 3 and online supplemental table 1). The mean potency values for B. arietans were variable, with some batches having distinct lower (1991 and 1997) or higher (2012 and 2015) potency, with the remainder having potency broadly spread in between (figure 3A). Overall, while significant differences in potency were notable between some batches, there was no correlation with the B. arietans venom neutralising ability with age or protein content. The majority of mean potency values of the expired antivenoms versus N. nigricollis and D. polylepis venoms were substantially lower than those versus B. arietans venom, in line with the well-described weaker capability of antivenoms in neutralising elapid venoms versus that of viper venoms (figure 3).41 The majority of expired antivenoms had potency values in the range of 0.6–1 mg/mL with substantially overlapping CIs against D. polylepis venom, while 2012 and 2017 expiry had notably greater potency (1.6 mg/mL) (figure 3B). As with the expired antivenom potency versus B. arietans venom, while significant differences in potency were notable between individual batches, overall, there was no correlation with D. polylepis venom neutralising ability with either age of the expired antivenom or its protein content. Expired antivenom potency versus N. nigricollis venom demonstrated remarkable consistency over time, with mean potency in the range of 0.6–1.1 mg/mL with broadly overlapping CIs, with no correlation with time of antivenom expiry or protein content (figure 3C).
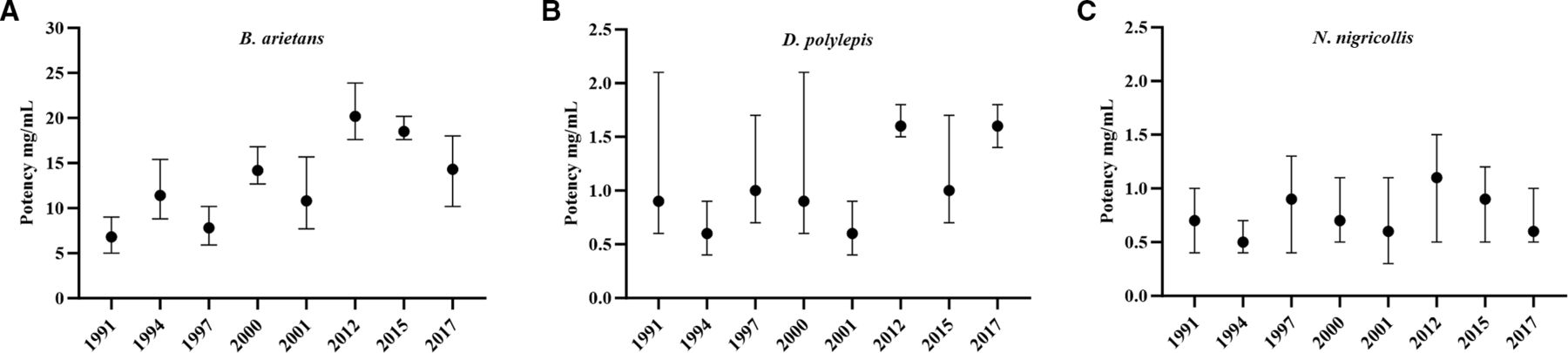
The ability of expired SAIMR polyvalent antivenoms to neutralise murine in vivo lethality. Antivenom expiry year is represented on each x axis. The ability to neutralise murine lethality is expressed as the median neutralising dose (ED50), presented as mg of venom neutralised per mL of antivenom (mg/mL) calculated by Probit analysis. Venoms tested were (A) Bitis arietans (vs 5× LD50), (B) Dendroaspis polylepis (vs 3× LD50) and (C) Naja nigricollis (vs 3× LD50). Error bars represent 95% Cls. For all experiments, each venom and antivenom dose were premixed, incubated at 37°C for 30 min before intravenous administration (n=5 mice/group). Results are representative of 6 hours post-venom injection. ED50, median effective dose; LD50, median lethal dose; SAIMR, South African Institute for Medical Research.
Discussion
In this study, we examined the immunochemical and preclinical neutralising efficacy of eight batches of expired SAIMR polyvalent antivenom, ranging from 6 to 32 years post-expiry, which had been kept in long-term refrigerated conditions, with the objective of inferring their potential suitability for use when alternatives are unavailable and to explore if existing expiry dates could be extended. The key finding of this study is that SAIMR polyvalent can retain the in vivo ability to neutralise murine venom-induced lethality for over 30 years; however, physical stability is limited to a shorter period of up to 25 years.
A major consideration for clinicians using antivenom is its visual appearance, with most clinicians unlikely to administer cloudy antivenoms for fear of loss of activity or increased likelihood of adverse reaction.42 In terms of physical stability, only the oldest antivenoms, which expired in 1991 and 1994, were visibly cloudy, with levels of turbidity in excess of permissible quality control levels. The turbidity is assumed to be aggregation of F(ab’)2, which does not represent a loss in neutralising capacity in some of the tests presented here, likely due to the majority of F(ab’)2 present in antivenom not being clinically relevant for envenoming,43 but is enough to increase turbidity substantially. Antivenom total protein concentration broadly remained stable over time, and SDS-PAGE analysis demonstrated comparable levels of F(ab’)2 fragments (figure 1C). However, minor differences in protein profiles were notable, indicating various levels of impurities, which we consider to be a result of normal manufacturing variability as opposed to deterioration in product.
Prior to in vivo assays, all antivenom batches were examined using in vitro immunological and biochemical assays to assess their ability to recognise and neutralise venom toxins. ELISA and immunoblots demonstrated all expired batches were able to recognise venoms, with no substantial differences in recognition based on antivenom expiry. Biochemical in vitro assays demonstrated that all antivenoms retained the ability to partially neutralise SVMP and PLA2-specific activity. Apparent decreases in SVMP and PLA2 neutralising activity for B. arietans and H. haemachatus were noted, with older expiring antivenoms inhibiting less toxin activity compared with antivenoms expiring more recently, although this trend was not apparent for N. nigricollis PLA2 activity. It is important to note that while these assays are a valuable indicator of whether an antivenom may or may not be suitable for use in vivo, thus preventing the use of mice in experiments likely to fail, they are not capable of predicting actual performance in vivo.
The results of the ED50 assay for determining the potency of each antivenom’s ability to neutralise the lethal effects of D. polylepis, N. nigricollis and B. arietans venom demonstrated all expired antivenoms retained preclinical efficacy, with no evidence of degradation of capability over time since expiry. The ED50 and potency values of the antivenoms versus D. polylepis and N. nigricollis are highly similar to that of previously reported values for these venoms,44–47 whereas the values for B. arietans are all within the range (higher end) of values previously reported.44 46–48 Importantly, the potency values for B. arietans and D. polylepis are highly similar to that established for a non-expired batch of SAIMR polyvalent (Batch BL01646, expiry May 2023) tested in 2021 versus B. arietans and D. polylepis venom from eSwatini (p=20.3 mg/mL and 1.8 mg/mL, respectively),44 suggesting that the in vivo potency of the expired antivenom batches is comparable with that of non-expired batches.
As described, many studies have demonstrated retained efficacy of expired antivenoms,17–19 and it is important to consider whether existing antivenom stocks could be used more efficiently,16 particularly given the lack of access to these products in low and middle-income settings.49–51 Reports suggest that clinicians are already using expired antivenom products due to lack of availability of in-date products,25 and the South-East Asia regional office WHO guidelines for managing snakebite endorse this in certain circumstances: ‘in patients with severe envenoming, recently expired antivenoms may be used if there is no alternative’.22 However, we must emphasise that while we and others have demonstrated retained preclinical efficacy of expired antivenoms in mouse models, the clinical efficacy and safety of these antivenoms cannot be confirmed from these assays. Expired antivenoms which are cloudy or have precipitates must not be administered due to the likely high risk of adverse reactions resulting from aggregates.52 The legal implications of prescribing expired antivenom must be emphasised, as the prescribing clinician may subsequently become liable for any adverse events suffered by the patient following administration of an expired antivenom and would need to counsel the patient on the potential risks.
Currently available antivenoms, particularly those marketed in Asia and Africa, are of varying quality and have often been approved by regulators and provisioned by health services, despite a lack of preclinical or clinical efficacy data.26 41 46 50 This lack of regulation has been disastrous, with evidence suggesting that poor-quality products have caused harm to patients.53 54 Some of the methods used in the present study are similar to those applied by the WHO antivenom risk–benefit assessment, which endeavours to exclude poor-quality products from the market. This programme includes a review of the product dossier, laboratory analysis (according to WHO standards for biological products)31 and manufacturing site inspection (to ensure adherence to Good Manufacturing Practices). Thus, it may be feasible for the WHO antivenom risk–benefit assessment to be extended to evaluate the quality and preclinical efficacy of expired products, which could enable manufacturers of good-quality antivenoms to extend the expiry date, or could provide regulators and clinicians with assurance that certain products can be administered for a defined period after their expiry date has passed. Preferentially, and following strengthening of regulatory systems in low/middle-income country settings, organisations such as the proposed African Medicines Agency55 could lead on ensuring the quality of antivenom products is acceptable, and on defining appropriate expiry dates.
There would be particular value in extending antivenom expiry dates if the proposed WHO antivenom stockpile for Africa were to become established.56 Efforts in the USA to stockpile medications that protect against certain public health emergencies,57 namely pandemics, have been hindered by the high costs of regularly replacing expired stockpiled products, which are carefully stored, but not used, for long periods of time. In response to this challenge, the FDA has provided various routes for products to be approved for use beyond their initial expiry date.58 Given that a regional stockpile of antivenom would entail storage of a large volume of product in a controlled environment, with appropriate temperature regulation, it is feasible that products could remain safe and effective beyond their expiration date, which could improve the financial viability of this important project. Additional in vivo preclinical evaluation of antivenom products would incur a substantial financial cost but given that antivenom products are expensive to produce,9 this may be cost-effective. The ethical cost of increasing what is already substantial and severe, in vivo preclinical testing would also have to be carefully considered. Many manufacturers will have run real time and accelerated stability studies on their antivenom products to explore what duration of time is acceptable for expiry (ie, beyond the listed expiry). Going forward, manufacturers could consider making these data available, such as described by Morokuma et al,20 to provide additional confidence in extended expiration.
Potential wider disincentives for manufacturers to pursue extension of antivenom expiry dates must be considered. The antivenom market has been fragile and manufacturers of higher-quality products have previously ceased production due to unsustainable economics,54 and there is a theoretical risk that extension of expiry dates could reduce product turnover and further impair financial sustainability. Nevertheless, by reducing waste of antivenom products, it is likely that manufacturers could adjust prices to offset losses while ultimately reducing the cost to health services and the public. The benefit of evaluating products based on quality, which has been pioneered by the WHO antivenom risk–benefit assessment, and removing poor products from the market, is a major step forward and should be further expanded to define evidence-based expiry dates.
A major limitation in this study is the absence of any non-expired SAIMR polyvalent for direct comparison. The reasoning behind this is twofold. First, SAIMR polyvalent is extremely expensive and notably extremely difficult to procure outside of South Africa, with anecdotal evidence of worsening supply issues recently. Second, due to these supply issues, we considered it unethical to use the highly limited quantity of SAIMR polyvalent available to us for research purposes, when they may be required in the event of an envenoming. Despite this, comparison with recent in vivo preclinical data available examining the efficacy of non-expired SAIMR polyvalent versus two similar venoms used in this study, demonstrating highly similar results,44 provides confidence in our conclusion that the expired antivenoms in this study have no demonstrable reduction in preclinical efficacy due to age.
Clearly, the older antivenoms used in this study (1991 and 1994 expiry) would not be considered for clinical use based on their appearance alone. Our results clearly suggest that the apparent instability associated with storage time is not reflected as a change in immunochemical properties or the neutralising potency, but as an increment of the turbidity. Reflecting this, antivenoms from 1997 onwards have favourable quality control profiles largely indistinguishable from what would be expected for in-date products. Therefore, we believe this study provides strong rationale for stakeholders (manufacturers, regulators and health authorities) to explore the use of expired antivenom and the extension of antivenom shelf life. The use of expired antivenom needs to be carefully assessed on a product-by-product and venom-by-venom basis, and confirmation of safety of such products is necessary. However, the evidence, both preclinical17–19 and clinical,21 23 25 demonstrating the long-term retained efficacy of antivenoms should lead to initiatives regarding changing expiry dates that could assist in alleviating chronic antivenom availability shortages globally.
[ad_2]
Source link